The Sugar–Kidney Trap (Why Early Kidney Damage Goes Undetected)
Most kidney damage does not begin with creatinine rise.
It begins with micro-glycemic toxicity, insulin resistance, and micro-vascular endothelial injury — which are only detected early by Cystatin-C, micro-albumin, and insulin markers.
Creatinine stays normal until >50% of nephrons are already destroyed.
1️⃣ Prediabetes Kidney Damage (Silent Nephropathy)
| Marker | Normal | Early Damage |
|---|---|---|
| Fasting Sugar | 98 | 104 |
| HbA1c | 5.4 | 5.8 |
| Creatinine | 0.9 | 0.9 (normal) |
| eGFR (creatinine) | 98 | 94 (appears normal) |
| Cystatin-C | 0.72 | 1.06 ⚠️ |
| Urine Microalbumin | 12 mg | 68 mg ⚠️ |
🧠 Meaning:
Sugar looks “borderline.” Kidneys are already leaking protein.
This person is already in Stage-1 Diabetic Nephropathy — undetected by creatinine.
2️⃣ Fatty Liver → Kidney Fibrosis Pathway
| Marker | Normal | Early Damage |
|---|---|---|
| ALT | 24 | 48 |
| Triglycerides | 110 | 220 |
| Fasting Insulin | 6 | 17 ⚠️ |
| Creatinine | 0.8 | 0.9 |
| Cystatin-C | 0.74 | 1.12 ⚠️ |
| eGFR (Cystatin) | 110 | 72 ⚠️ |
🧠 Meaning:
Fatty liver and insulin resistance are silently scarring kidneys — years before CKD diagnosis.
3️⃣ Hypertension-Induced Kidney Damage (Normal Creatinine Trap)
| Marker | Normal | Early Damage |
|---|---|---|
| BP | 118/76 | 138/86 |
| Fasting Sugar | 92 | 101 |
| Creatinine | 1.0 | 1.0 |
| eGFR (creatinine) | 92 | 91 |
| Cystatin-C | 0.77 | 1.19 ⚠️ |
| Urine Albumin | 9 mg | 82 mg ⚠️ |
🧠 Meaning:
Blood pressure is silently destroying glomeruli while creatinine hides it.
4️⃣ “Normal Sugar” Kidney Disease (The Dangerous Zone)
| Marker | Normal | Early Damage |
|---|---|---|
| Fasting Sugar | 90 | 95 |
| HbA1c | 5.2 | 5.5 |
| Creatinine | 0.9 | 0.9 |
| Cystatin-C | 0.70 | 1.03 ⚠️ |
| Urine Microalbumin | 7 mg | 61 mg ⚠️ |
🧠 Meaning:
This is non-diabetic kidney disease — driven by sugar spikes, insulin resistance, and oxidative stress.
5️⃣ The Missed Opportunity Zone
These patients look normal.
They are not normal.
They are already in reversible kidney injury.
Once creatinine rises — the damage is permanent.
The Marker Doctors Rarely Order
🔬 CYSTATIN-C
• Detects kidney injury 5–8 years earlier
• Not affected by muscle mass
• Detects micro-vascular nephron loss
• Predicts dialysis risk decades earlierKidney Disease Begins Long Before Lab Results Change
Chronic kidney disease (CKD) rarely begins with pain, swelling, or abnormal creatinine levels.
By the time routine kidney tests appear abnormal, more than 50% of kidney function may already be lost — and that damage is often permanent.
Modern biomarker science now allows detection of silent kidney injury years before diagnosis, giving patients the opportunity to prevent kidney failure rather than manage it.
Why Routine Kidney Tests Miss Early Damage
Standard kidney panels focus on late-stage filtration failure:
• Serum creatinine
• eGFR
• Urine protein
These rise only after significant nephron loss.
Early kidney injury begins with micro-inflammation, vascular injury, and tubular stress — invisible on routine labs.
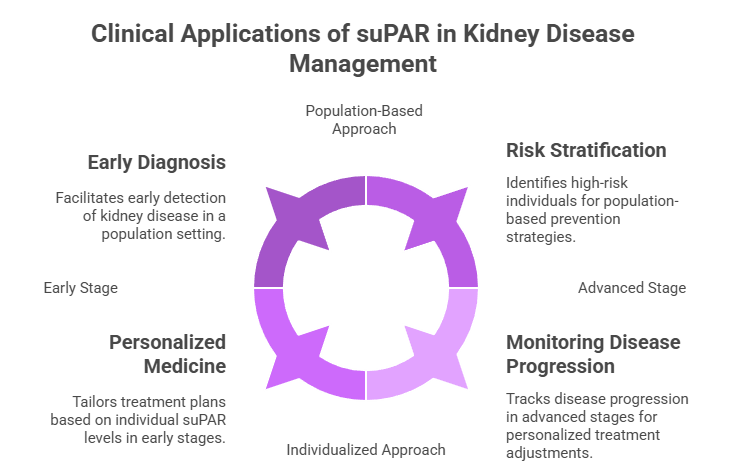
The Marker Changing Preventive Nephrology: suPAR
suPAR (soluble urokinase plasminogen activator receptor) is one of the strongest predictors of early kidney disease.
Elevated suPAR predicts:
• Progressive kidney decline
• Dialysis risk
• Cardiovascular mortality
• Diabetes-related nephropathy
Years before creatinine rises.
Additional Early Kidney Damage Markers
| Biomarker | What It Detects |
|---|---|
| Cystatin-C | Early filtration decline |
| KIM-1 | Tubular cell injury |
| NGAL | Acute and chronic kidney stress |
| Homocysteine | Vascular kidney injury |
| Uromodulin | Tubular integrity |
These provide a multi-layered view of renal health.
Who Should Be Screened Early?
• Adults over 30
• People with diabetes or hypertension
• Individuals with family history of kidney disease
• Those with fatigue, swelling, or frequent infections
Early Detection Prevents Dialysis
Early kidney injury is often reversible when detected early:
• Blood pressure optimization
• Glucose control
• Anti-inflammatory nutrition
• Weight management
• Hydration correction
Conclusion
Kidney failure does not begin with abnormal labs — it begins silently.
Early biomarkers allow prevention instead of dialysis.
Medical Disclaimer
Educational only. Consult your physician before testing.