

Understanding GLP-1 and Semaglutide
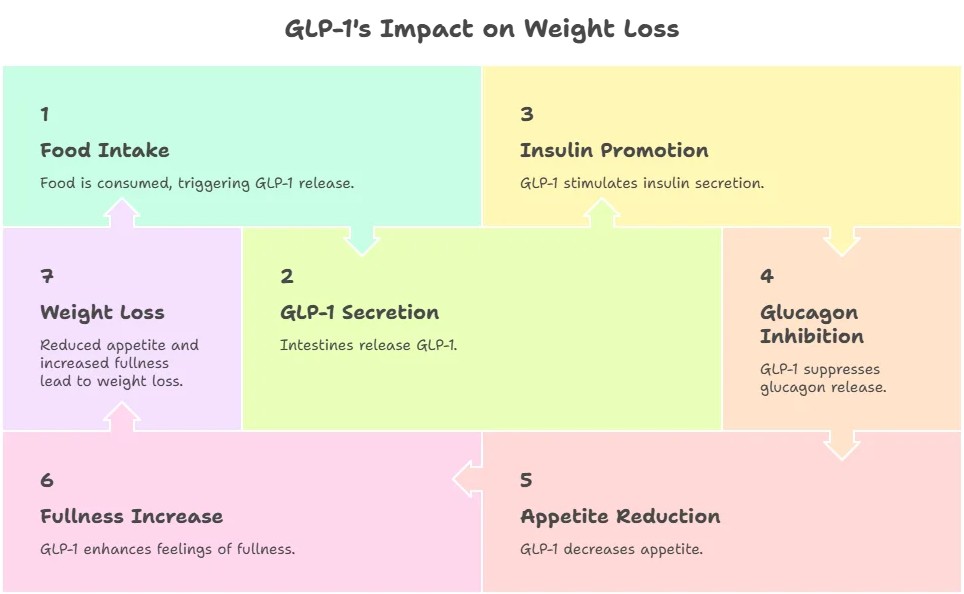
GLP-1, or glucagon-like peptide-1, is a hormone that plays a crucial role in glucose metabolism and appetite regulation. It is secreted by the intestines in response to food intake, promoting insulin secretion while inhibiting glucagon release. Semaglutide mimics the action of GLP-1, leading to reduced appetite and increased feelings of fullness, which can significantly aid in weight loss.
GLP-1 Weight Loss Breakthrough
Complete USA FAQ Guide – 100 Questions Answered (March 2026 Edition) | IntelliNewz – Evidence-Based Insights for Americans
1. What is GLP-1 and how does it work for weight loss?
2. What does GLP-1 stand for?
3. How do GLP-1 receptor agonists help reduce appetite?
4. Why are GLP-1 medications considered a breakthrough?
5. Are GLP-1 drugs approved for obesity?
6. What makes GLP-1 medications different from diet pills?
7. Are GLP-1 drugs hormones?
8. Do GLP-1 medications affect metabolism?
9. How do they impact insulin levels?
10. Are these medications safe for long-term use?
11. What is semaglutide?
12. How does tirzepatide work?
13. Is Wegovy different from Ozempic?
14. What is Mounjaro used for?
15. Are there triple-agonist weight loss drugs available yet?
16. Which GLP-1 medication causes the most weight loss?
17. Are generic GLP-1 medications available?
18. What is the difference between injectable and oral GLP-1 drugs?
19. Is oral semaglutide effective for weight loss?
20. How often are GLP-1 injections given?
21. Who qualifies for GLP-1 weight loss medication?
22. Can someone with a BMI under 27 use GLP-1 drugs?
23. Are GLP-1 medications only for people with diabetes?
24. Can people with PCOS use GLP-1 therapy?
25. Are GLP-1 drugs safe for seniors?
26. Can teenagers use GLP-1 medications?
27. Are they safe during menopause?
28. Can someone with thyroid disease take GLP-1?
29. Who should NOT take GLP-1 medications?
30. Is a prescription required?
31. How much weight can you lose on GLP-1 drugs?
32. How fast does weight loss begin?
33. Is weight loss sustained long term?
34. What percentage of body weight is typically lost?
35. Does the weight come back after stopping?
36. Are results better than bariatric surgery?
37. How long should treatment continue?
38. Do GLP-1 drugs reduce belly fat?
39. Do they improve metabolic health markers?
40. Can they reverse insulin resistance?
41. What are the most common side effects?
42. Why do GLP-1 drugs cause nausea?
43. How long does nausea last?
44. Can they cause vomiting?
45. Do GLP-1 medications cause hair loss?
46. Can they lead to muscle loss?
47. Are gallbladder issues common?
48. Do GLP-1 drugs increase pancreatitis risk?
49. What is the thyroid cancer warning about?
50. Are there long-term safety concerns?
51. Are GLP-1 drugs FDA approved for weight loss?
52. What warnings do they carry?
53. Can they cause low blood sugar?
54. Are they safe with blood pressure medication?
55. Can they affect heart rate?
56. Are they safe for people with heart disease?
57. What lab tests are needed before starting?
58. How often should monitoring occur?
59. Can they be used with other weight loss drugs?
60. What happens in case of overdose?
61. How much do GLP-1 medications cost?
62. Does insurance cover them?
63. Are they covered for obesity without diabetes?
64. Can they be compounded?
65. Are compounded versions safe?
66. How are injections administered?
67. Do they need refrigeration?
68. What happens if you miss a dose?
69. Can you travel with GLP-1 injections?
70. Do they interact with alcohol?
71. Do you still need to diet while on GLP-1?
72. Is exercise required?
73. What diet works best with GLP-1 therapy?
74. Do they reduce cravings?
75. Can you eat normally?
76. Do they affect taste preferences?
77. Can you build muscle while using them?
78. Should protein intake be increased?
79. Do they help emotional eating?
80. Can they improve sleep apnea?
81. What happens when you stop GLP-1 medication?
82. Is maintenance dosing required?
83. Can dosage be reduced after goal weight?
84. Do hunger levels return?
85. Is tapering necessary?
86. Can you restart after stopping?
87. Are there withdrawal symptoms?
88. Do they slow metabolism long term?
89. Is lifelong treatment recommended?
90. What do experts recommend in 2026?
91. Are GLP-1 drugs just a trend?
92. Are celebrities using GLP-1 secretly?
93. Is this “cheating” weight loss?
94. Do they cause facial aging (“Ozempic face”)?
95. Can they cause depression?
96. Are they addictive?
97. Do they shrink your stomach?
98. Are they safe for athletes?
99. Is rapid weight loss dangerous?
100. Are GLP-1 medications truly the future of obesity treatment?
Semaglutide was initially developed for the treatment of type 2 diabetes but has since been recognized for its weight loss benefits. In 2021, the FDA approved semaglutide for chronic weight management in adults with obesity or overweight conditions, marking a significant milestone in obesity treatment.
If you’ve scrolled through social media, watched the news, or talked to friends lately, you’ve probably heard about a class of drugs that seems to be everywhere: GLP-1s. From Ozempic to Wegovy, these medications have transformed how we think about weight loss. But with all the buzz comes confusion. What exactly are these drugs? Did Elon Musk really use them? And most importantly—do they actually work?
Let’s answer the questions Americans are actually asking.
What Does “GLP-1” Even Stand For?
Let’s start with the basics. GLP-1 stands for glucagon-like peptide-1. It’s a mouthful, but here’s what you need to know: GLP-1 is a natural hormone your gut produces that helps regulate blood sugar and appetite. These medications mimic that hormone, essentially tricking your body into feeling fuller longer and producing more insulin when you eat .
Think of it as boosting a system your body already has in place—just giving it some extra help.
What Are GLP-1 Drugs Made For?
Originally, these medications were developed for one primary purpose: treating type 2 diabetes. The first GLP-1 drug, exenatide (Byetta), was approved for diabetes in 2005.
But here’s where things got interesting. Patients kept reporting something unexpected: they were losing weight. Significantly. This observation sent researchers down a path that would eventually revolutionize obesity treatment.
Today, GLP-1s are approved for multiple conditions:
- Type 2 diabetes (Ozempic, Rybelsus, Victoza)
- Weight management (Wegovy, Saxenda, Zepbound)
- Cardiovascular risk reduction in people with heart disease
- Obstructive sleep apnea (tirzepatide was approved for this in December 2024)
- Chronic kidney disease risk reduction (semaglutide approved January 2025)
- Metabolic dysfunction-associated steatohepatitis (MASH) , a serious liver disease

And researchers aren’t stopping there. Current studies are exploring benefits for Alzheimer’s disease, Parkinson’s, addiction, and even osteoarthritis.
When Were GLP-1s First Approved for Diabetes?
The timeline matters here because it shows how long these drugs have actually been studied:
- 2005: Exenatide (Byetta) becomes the first GLP-1 approved for type 2 diabetes
- 2010: Liraglutide (Victoza) approved for diabetes
- 2014: Dulaglutide (Trulicity) approved
- 2017: Semaglutide (Ozempic) approved for diabetes
- 2019: Oral semaglutide (Rybelsus) becomes the first oral GLP-1 for diabetes
So while it feels like these drugs exploded overnight, researchers have been studying them for two decades.
When Was the First GLP-1 Approved for Weight Loss?
This is where the story shifts. The first GLP-1 approved specifically for weight loss was liraglutide (Saxenda) in 2014. But it was semaglutide—at a higher dose than the diabetes version—that truly captured public attention when Wegovy was approved for weight management in 2021.
Then came tirzepatide (Zepbound) in 2023, approved for weight loss after showing impressive results.
So… Which GLP-1 Is Actually Best for Weight Loss?
This is the million-dollar question. According to the most recent research, the answer depends on whether you want what’s available now or what’s coming soon.
For currently available medications, tirzepatide (Mounjaro/Zepbound) ranks highest. A major 2025 network meta-analysis presented at the American Heart Association found that among commercially available agents, tirzepatide achieved the greatest weight reduction. It’s a “dual agonist,” meaning it targets both GLP-1 and another hormone called GIP.
Semaglutide (Wegovy/Ozempic) comes next, followed by liraglutide (Saxenda). Here’s how they stack up:
- Tirzepatide: ~9.6% weight loss at 6 months (at highest doses)
- Semaglutide: Significant weight loss, though less than tirzepatide
- Liraglutide: Modest weight loss (~6% body weight)
But here’s what’s coming: Experimental drugs like retatrude (a “triple agonist”) are showing jaw-dropping results—up to 24.2% weight loss in clinical trials, which approaches what you’d see with bariatric surgery.
Is Ozempic a GLP-1?
Yes. Ozempic is absolutely a GLP-1—specifically, it’s the brand name for semaglutide when prescribed for type 2 diabetes. The same active ingredient in a different dose becomes Wegovy when prescribed for weight loss.
This confusion has led to off-label prescribing and, at times, shortages that frustrated patients with diabetes who actually needed the medication.
Did Elon Musk Use Semaglutide?
Yes, essentially. When Elon Musk dramatically transformed his physique, speculation ran wild. Musk himself confirmed he used “Wegovy” —which contains semaglutide, the exact same active ingredient as Ozempic.
Plastic surgeons and weight loss experts interviewed by DailyMail.com noted that his transformation was “particularly jarring” and likely involved a combination of the medication, fasting, and working with a trainer. Dr. Jordan Terner, a plastic surgeon, commented: “He looks good. He definitely looks chiseled and fresh… I know he has definitely admitted to using a semaglutide.”
Of course, experts also noted he’s likely combined the medication with significant lifestyle changes, weight training, and possibly even cosmetic procedures to address what’s been dubbed “Ozempic face”—the gaunt appearance that can result from rapid weight loss.
Is the Wegovy Pill Cheaper Than the Injection?
This is a practical question for anyone considering these medications. The answer has changed dramatically recently.
Current pricing (as of early 2026) : For cash-paying patients, the Wegovy pill starts at $149 per month for the lowest doses, while the injection starts at $199 per month for new patients. After the first two months, prices rise to $349 for the pill and $299 for the injection.
These are self-pay prices through manufacturer savings programs—not valid with insurance. Commercially insured patients with coverage might pay as little as $25 for a prescription.
Without these programs, list prices range from $500 to over $1,300 monthly. This has led some insurance plans to limit coverage, and CMS (Centers for Medicare & Medicaid Services) does not cover weight loss drugs at all.
Do GLP-1s Really Work for Weight Loss?
This might be the most important question, and the evidence is overwhelming: yes, GLP-1s genuinely work for weight loss—but with important caveats.
Clinical trials show consistent, significant results:
- In the STEP-HFpEF trial, semaglutide led to 13.3% weight loss compared to 2.6% with placebo
- A 2025 New England Journal of Medicine study on orforglipron (an experimental oral GLP-1) showed up to 11.2% weight loss at 72 weeks, with 18.4% of patients losing 20% or more of their body weight
- Tirzepatide trials have shown remarkable efficacy for both diabetes and weight management
But “work” means more than just losing pounds. These medications improve waist circumference, blood pressure, triglyceride levels, and non-HDL cholesterol. They’re transforming how we treat obesity as a chronic disease, not just a lifestyle issue.
What About GLP-1 Supplements?
This is where things get murky—and where consumers need to be extremely careful. With the explosion of interest in GLP-1 drugs, supplement manufacturers have rushed to market with products claiming to offer similar benefits. But experts at Harvard T.H. Chan School of Public Health warn that these supplements do not come close to matching the effectiveness of real GLP-1 agonists .
Two Very Different Categories of Supplements
It’s important to understand that there are actually two distinct types of products being marketed as “GLP-1 supplements”:

1. Supplements claiming to boost natural GLP-1 production. These products contain ingredients that manufacturers claim will stimulate your body’s own GLP-1 production. Common ingredients include berberine, curcumin, probiotics, omega-3 fatty acids, green tea extract, and various botanical extracts .
2. Supplements designed for people already taking GLP-1 medications. A newer category has emerged that doesn’t claim to replace GLP-1 drugs but rather to support users by addressing side effects and nutritional gaps. These include protein powders, fiber supplements, creatine for muscle preservation, and specialized multivitamins .
What the Research Actually Shows
Some emerging research suggests certain ingredients may influence GLP-1 levels:
- Berberine, a compound found in certain plants, may improve how your body uses sugar by activating metabolic pathways, and some studies suggest three 500-mg doses per day may be effective .
- Curcumin (turmeric’s active ingredient) may help increase GLP-1 levels by improving gut health and reducing inflammation .
- Probiotics, particularly certain strains, may boost GLP-1 activity, though researchers haven’t identified a single most effective strain .
- Botanical extracts like Dichrostachys glomerata and Cissus quadrangularis showed promise in a 16-week clinical trial, with participants experiencing 5% or greater weight loss and increased GLP-1 levels—though results still didn’t match semaglutide .
However, experts urge extreme caution in interpreting these findings. Dr. Mir Ali, a bariatric surgeon, told Women’s Health: “I haven’t seen convincing evidence that any of these will make a significant impact on weight loss. They are not nearly on par with weight loss medications” .
The Regulatory Reality
Here’s the critical thing to understand: dietary supplements are not regulated like drugs. Under the Dietary Supplement Health and Education Act (DSHEA) of 1994, supplements do not require premarket approval from the FDA . Manufacturers are responsible for their own safety and labeling, and the FDA typically only steps in after problems arise.
This has led to some concerning situations:

- The FDA prohibits marketing supplements in ways that suggest they work as well as or better than GLP-1 drugs .
- Some products use deceptive advertising or lack required FDA disclaimers .
- A 2026 analysis identified 24 transdermal patch “GLP-1” supplements that are actually illegal, as dietary supplements must be swallowed, not applied to skin .
- Many products have 1- to 2-star reviews with consumer comments suggesting lack of efficacy or adverse events .
What About the “Support” Supplements?
For the second category—supplements designed for people already on GLP-1 medications—the picture is different. These products address legitimate concerns:
- Muscle loss: Up to 40-60% of weight loss during GLP-1 use can come from muscle, making protein and creatine supplementation potentially valuable .
- Constipation: A persistent side effect that targeted biotics may help address .
- Nutrient deficiencies: Reduced food intake can lead to gaps in vitamins and minerals .
The Vitamin Shoppe recently launched an entire line of GLP-1 support supplements, including meal-replacement powders, fiber supplements, and collagen for skin health . These don’t claim to boost GLP-1—they simply help users stay healthy while on the medication.
The Bottom Line on Supplements
If you’re considering GLP-1 supplements, here’s what experts want you to know:
- Be skeptical of any product claiming to work “like Ozempic” or “naturally” produce the same results .
- Look for third-party testing from organizations like NSF International, USP, or ConsumerLab .
- Consult your doctor before starting any supplement, especially if you take other medications .
- Focus on proven strategies first: Dr. Ali notes that eating more protein (1.2 to 1.5 grams per kilogram of body weight daily) naturally increases GLP-1 production .
- Understand the legal limits: Supplements cannot claim to treat, prevent, or cure diseases like diabetes or obesity .
As Bryn Austin of Harvard put it: “Any consumer seeing the kind of marketing and claims on packages would likely infer that many of them do have those effects”—even when the evidence doesn’t support it .
Who Discovered GLP-1? (The Nobel Prize Story)
This question reveals a fascinating scientific detective story that’s very much still unfolding.
The key discoverers are Drs. Joel Habener and Svetlana Mojsov, who identified and characterized the GLP-1 hormone in the 1980s at Massachusetts General Hospital. Dr. Lotte Knudsen later led the team at Novo Nordisk that created the first GLP-1-mimicking drug approved for obesity.
Have they won a Nobel Prize? Not yet—but they’ve been sweeping every major award that often precedes one. In September 2024, Habener, Mojsov, and Knudsen received the prestigious Lasker-DeBakey Clinical Medical Research Award. As Mariana Lenharo wrote in Nature, “Receiving these awards often precedes a Nobel Prize.”
Other giants in the field include Daniel Drucker, Jens Holst, and Graeme Bell, who’ve collectively received the Warren Alpert Prize (2020), Gairdner International Award (2021), Wolf Prize (2023), and Tang Prize (2024).
As one researcher put it: “It’s 10,000 ants that move the anthill, and we are trying to pick out the three ants that made the most differences.”
Can You Get GLP-1s Online?
Yes, but proceed with caution. Many telehealth companies now offer GLP-1 prescriptions after online consultations. However:
- Legitimate providers require actual medical evaluation, not just a questionnaire
- Compounded versions (custom-mixed drugs) exist but face legal challenges from manufacturers and regulatory scrutiny
- Safety concerns are real—without proper oversight, you risk incorrect dosing or contaminated products
If you’re considering this route, ensure the provider is licensed in your state, requires lab work or medical records, and doesn’t just rubber-stamp prescriptions.
The Bottom Line
GLP-1 medications represent a genuine revolution in treating obesity and related conditions. They’re not magic—they require commitment, come with potential side effects, and work best alongside healthy lifestyle changes. But for millions of Americans struggling with weight, they offer something previously unavailable: a medication that actually targets the underlying biology of obesity.
When it comes to supplements, let the buyer beware. While some may offer modest support—either by potentially influencing GLP-1 levels or by helping medication users stay healthy—none come close to matching prescription GLP-1s. If a product sounds too good to be true, it probably is.
The science continues evolving rapidly. New drugs in the pipeline promise even greater efficacy, and researchers are exploring benefits for conditions from heart failure to Alzheimer’s. What started as a diabetes treatment has become one of the most important medical developments of our time.
As always, if you’re considering GLP-1s or supplements to support your health journey, talk to your doctor. These are prescription medications for a reason—they require medical supervision to ensure they’re right for you and safe for your specific health situation.
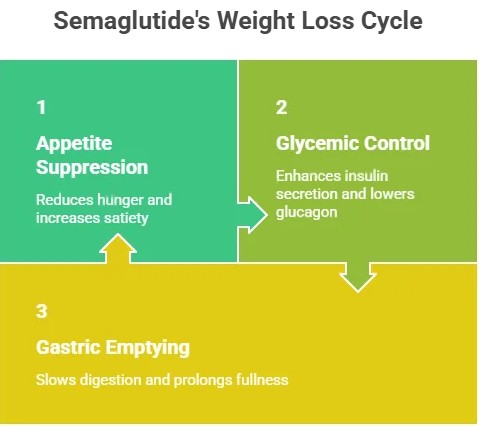
Mechanism of Action
Semaglutide works through several mechanisms:
- Appetite Suppression: By acting on the brain’s appetite control centers, semaglutide reduces hunger and increases satiety, leading to lower caloric intake.
- Glycemic Control: It enhances insulin secretion in response to meals and lowers glucagon levels, which helps regulate blood sugar levels.
- Gastric Emptying: Semaglutide slows gastric emptying, prolonging the feeling of fullness after meals.
These combined effects contribute to significant weight loss and improved metabolic health.
Clinical Efficacy
Clinical trials have demonstrated the effectiveness of semaglutide in promoting weight loss. In the STEP (Semaglutide Treatment Effect in People with Obesity) trials, participants receiving semaglutide experienced an average weight loss of approximately 15-20% of their body weight over 68 weeks. This is a substantial improvement compared to placebo groups, which saw minimal weight loss.
In 2026, ongoing studies continue to support the long-term efficacy of semaglutide, with many participants maintaining significant weight loss even after discontinuation of the medication. This suggests that semaglutide not only aids in initial weight loss but also helps in sustaining weight loss over time.
Safety and Tolerability
Safety is a paramount concern in any weight loss intervention. Semaglutide has been shown to have a favorable safety profile. Common side effects include gastrointestinal issues such as nausea, vomiting, and diarrhea, which often diminish over time as the body adjusts to the medication. Serious side effects are rare but can include pancreatitis and thyroid tumors.
In 2026, ongoing monitoring and post-marketing studies continue to assess the long-term safety of semaglutide, providing reassurance to both healthcare providers and patients.
Accessibility and Future Directions
As of 2026, semaglutide is becoming increasingly accessible to patients seeking effective weight management solutions. Insurance coverage for obesity medications is improving, and healthcare providers are becoming more knowledgeable about the benefits of GLP-1 receptor agonists.
Looking ahead, research is ongoing to explore the potential of semaglutide in various populations, including adolescents and individuals with different comorbidities. Additionally, combination therapies that pair semaglutide with lifestyle interventions may enhance weight loss outcomes and improve overall health.
Medical Disclaimer – IntelliNewz
The information provided by IntelliNewz is for educational and informational purposes only and is not intended as medical advice, diagnosis, or treatment. The content published on this website does not replace professional consultation with a licensed physician, healthcare provider, or qualified medical specialist.
GLP-1 medications and other prescription treatments should only be used under direct medical supervision. Individual results may vary based on medical history, existing conditions, and adherence to treatment plans.
Never disregard professional medical advice or delay seeking care because of something you have read on this website. If you believe you are experiencing a medical emergency, contact your doctor, local emergency services, or dial 911 immediately.
IntelliNewz does not assume responsibility for outcomes resulting from the use of information provided on this site. Readers are encouraged to consult a qualified healthcare professional before starting, stopping, or modifying any medication or treatment.
Content may be updated periodically as new research becomes available.
© IntelliNewz Health Desk

