
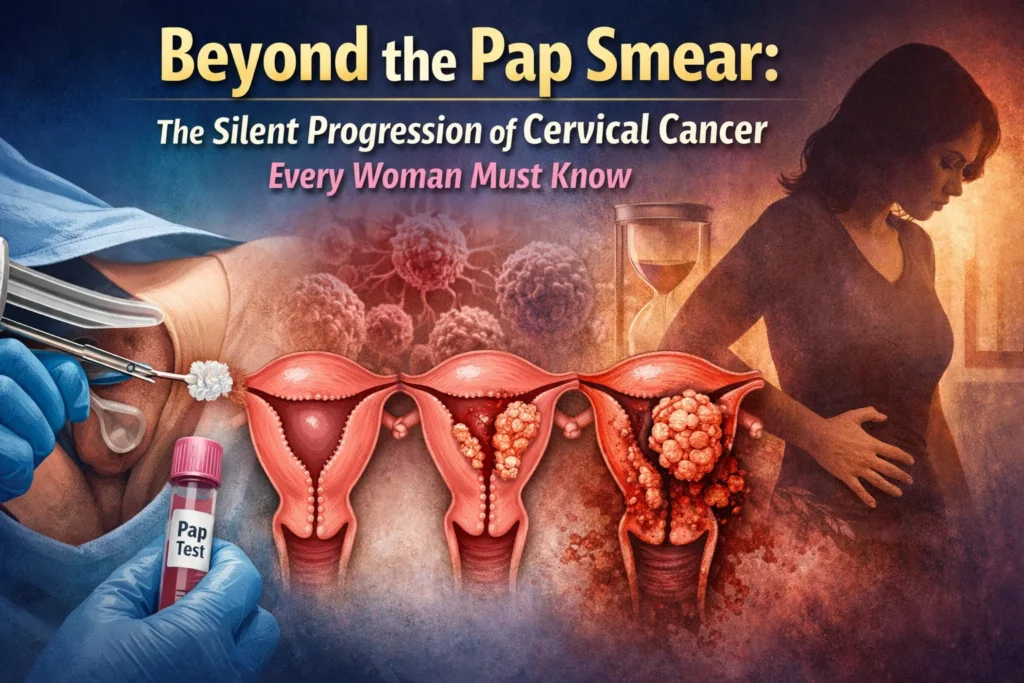
When we talk about cancer of the cervix, we are discussing one of the most preventable yet persistently dangerous cancers affecting women worldwide. Unlike many other malignancies, this cancer has a long pre-cancerous stage, meaning that if we understand the signs and the science, we have a massive window to stop it. To truly grasp this disease, we must look beyond a single picture of cervix cancer—which often shows a lesion that looks like an angry, irregular ulceration—and understand the biology, the spread, and the subtle symptoms that are frequently dismissed.
The Anatomy: Uterus vs. Cervix
To understand the pathology, one must distinguish between cancer of uterus and cervix. The cervix is the narrow, lower passageway that connects the uterus (the womb) to the vagina. While they are adjacent, cancers in these two locations behave very differently. Cancer of the cervix is almost always caused by persistent infection with high-risk strains of human papillomavirus (HPV). In contrast, cancer of the uterus (endometrial cancer) is usually linked to hormonal imbalances and often announces itself early with bleeding. This distinction is critical because the treatment pathways diverge entirely.
The Silent Invader: Symptoms and Spread
One of the most dangerous aspects of this disease is that early cancer of the cervix or uterus symptoms can be non-existent. When symptoms do appear, they are often mistaken for benign issues:
- Abnormal bleeding: Bleeding between periods, after intercourse, or after menopause.
- Unusual discharge: Watery, pink, or foul-smelling discharge.
- Pain: Pelvic pain or pain during intercourse.
If left untreated, the disease progresses. A common and frightening question is, where does cancer of the cervix spread to? It typically follows a predictable, stepwise pattern. Locally, it invades the parametrium (the tissues around the uterus). As it advances, it spreads to the pelvic lymph nodes, then the para-aortic lymph nodes. In later stages, it can metastasize to distant organs such as the lungs, liver, or bones.
The Gray Area: In Situ and Rare Variants
A point of confusion for many patients is the classification of non-invasive disease. Is adenocarcinoma in situ of cervix considered cancer? Technically, the answer is nuanced. “In situ” means “in its original place.” While it is a high-grade abnormality where abnormal cells are present but have not yet broken through the basement membrane to invade deeper tissues, it is considered a pre-cancer. It is treated aggressively (usually with a cone biopsy) to prevent it from becoming invasive cancer, but it is not staged as invasive cancer of the cervix.
There are also rare, aggressive subtypes. Clear cell cancer of the cervix is a notable variant. Unlike the common squamous cell carcinomas linked to HPV, clear cell adenocarcinoma is often not associated with HPV. It gained notoriety for being linked to in utero exposure to diethylstilbestrol (DES), a drug prescribed to pregnant women decades ago. It requires specialized treatment due to its unique resistance to standard chemotherapy protocols.
The Blueprint: Staging the Disease
Once a diagnosis of invasive cancer is confirmed, the medical community relies on a standardized system to determine prognosis and treatment. The FIGO staging of cancer cervix (International Federation of Gynecology and Obstetrics) is the gold standard. Unlike many other cancers that rely heavily on surgery for staging, cervical cancer is staged clinically, meaning doctors use examination, imaging, and biopsies to categorize the extent.
- Stage I: The cancer is strictly confined to the cervix.
- Stage II: The cancer has spread beyond the cervix but not to the pelvic wall or the lower third of the vagina.
- Stage III: The cancer extends to the pelvic wall, involves the lower vagina, or causes kidney problems (hydronephrosis).
- Stage IV: The cancer has spread beyond the pelvis to the bladder, rectum, or distant organs.
- Prevention and Precautions: Taking Control of Your Cervical Health
Given the silent nature of cancer of the cervix, relying on symptoms alone is a dangerous gamble. The good news is that cervical cancer is one of the few malignancies for which we have a clear roadmap for prevention. The precautions one needs to take care of fall into three distinct categories: vaccination, screening, and lifestyle vigilance.
1. Vaccination: The First Line of Defense
The most powerful precaution against cancer of the cervix is the HPV vaccine. Since persistent high-risk HPV is the cause of over 99% of cervical cancers, preventing the infection effectively prevents the cancer.
Who should take it: While ideally administered to preteens (ages 9–12), it is approved for adults up to age 45. Even if you are already sexually active, the vaccine can protect against the strains of HPV you haven’t encountered yet.
Why it matters: It protects against HPV 16 and 18, which are responsible for the majority of cases, including the glandular types like adenocarcinoma in situ of cervix.
2. Screening: The Non-Negotiable Routine
You cannot feel pre-cancer. By the time there is a visible abnormality on a picture of a cervix with cancer, the disease may have been developing for years. The precaution here is adherence to screening schedules regardless of symptoms.
Pap Smear (Pap Test): This detects abnormal cells before they become invasive. It can catch adenocarcinoma in situ (the pre-cancerous stage) early enough to remove it with a simple procedure, preserving fertility.
HPV Testing: This looks for the virus itself.
The Guideline: Generally, women should start screening at age 21. If results are normal, tests are typically repeated every 3 to 5 years. Do not skip these appointments just because you feel “fine.”
3. Recognizing Red Flags (Despite Negative Tests)
While rare, there are aggressive subtypes, such as clear cell cancer of the cervix, that can sometimes be missed by standard Pap smears because they arise in the cervical canal (glandular tissue) rather than the outer surface. Similarly, cancer of uterus and cervix (either primary or co-existing) can present with symptoms even if a recent Pap was normal.
The Precaution: Do not dismiss bleeding. If you experience bleeding after intercourse, bleeding between periods, or unusual watery discharge, insist on further evaluation—even if your last Pap smear was normal. You may need an ultrasound or an endometrial biopsy to rule out cancer of the uterus or a rare cervical variant.
4. Lifestyle and Risk Reduction
While HPV is the primary cause, co-factors can determine whether the infection clears up on its own or progresses to invasive cancer of the cervix.
Smoking Cessation: Tobacco byproducts are concentrated in the cervical mucus. Smokers are twice as likely to develop squamous cell cervical cancer compared to non-smokers.
Immune Health: A robust immune system usually clears HPV within 1–2 years. Managing stress, maintaining a healthy diet, and managing autoimmune conditions (or HIV) are crucial precautions to prevent the virus from persisting.
Safe Practices: Using barrier protection (condoms) reduces the risk of HPV transmission and protects against other sexually transmitted infections that can cause cervical inflammation, making the cervix more vulnerable to persistent infection.
5. Understanding the “Where” and “Why” of Vigilance
To take proper precautions, one must understand where does cancer of the cervix spread to if ignored. It spreads locally to the parametrium, then to lymph nodes, and finally to the lungs and liver. Knowing this progression reinforces why early detection is critical. Once the disease moves beyond the cervix, the treatment shifts from minor surgical excision to radical hysterectomy, radiation, and chemotherapy—a journey that is far more grueling than routine screening.
Summary of Precautions
Precaution
Action
Vaccination
Discuss the HPV vaccine with your doctor; it’s not just for teenagers.
Regular Screening
Adhere to FIGO staging prevention by catching lesions at Stage 0 (pre-cancer) via Pap/HPV co-testing.
Symptom Vigilance
Treat any abnormal bleeding as a medical priority, regardless of recent test results.
Lifestyle
Quit smoking; maintain immune health to help the body clear HPV infections.
Taking these precautions ensures that you never have to look at a picture of cervix cancer and wonder if it could have been prevented. In the vast majority of cases, it can be.
If you were to look at a picture of a cervix with cancer, you would rarely see a “normal” looking cervix. In cases of invasive squamous cell carcinoma, the transformation zone (where the glandular cells meet the squamous cells) often shows a visible mass. It might appear as a raised, ulcerated area that bleeds easily upon touch. In contrast, adenocarcinoma (which arises from the glandular cells) can sometimes hide inside the cervical canal, making it harder to visualize without an MRI or endocervical curettage.
Conclusion
The journey from an abnormal cell to a FIGO staging of cancer cervix Stage IV diagnosis is long—often spanning a decade. This timeline is our greatest weapon. While a picture of cervix cancer may look frightening, the reality is that regular screening (Pap smears and HPV testing) can detect the changes long before a tumor forms. Understanding the difference between uterine and cervical symptoms, recognizing the risk of rare variants like clear cell cancer, and knowing that adenocarcinoma in situ is a critical warning sign rather than an invasive crisis, empowers women to seek care early.
Do not wait for the symptoms of advanced disease to appear. If you experience any unusual bleeding or pelvic pain, demand answers. In the fight against cancer of the cervix, knowledge and early detection remain the ultimate cure.
This response is AI-generated, for reference o

