Table of contents
9 essential facts to reduce weight regain & recover smarter
These nine pillars form the backbone of a smarter recovery — reducing regain by up to 40% in observational studies.
Comparative study · Tirzepatide vs. after stopping
During tirzepatide
- Strong GIP/GLP-1 dual agonism → satiety, delayed gastric emptying
- Average weight loss 15–20% (SURMOUNT trials)
- Fat loss > lean loss (if protein + resistance)
- GI side effects (nausea, vomiting) more common at titration
After stopping tirzepatide
- Appetite rebound within 2–4 weeks
- Weight regain: ~50% of lost weight at 1 year (SURMOUNT-4)
- Possible transient joint aches, fatigue, GI flare
- Muscle loss can accelerate if training stops
Key insight: tirzepatide produces superior weight loss vs semaglutide, but post-discontinuation metabolic adaptation is similar – planning a maintenance phase is critical.
Body composition & muscle · what you need to know
Does tirzepatide change body composition? Yes. It preferentially reduces fat mass, especially visceral fat, while preserving lean mass — provided protein intake and resistance training are adequate.
Is it possible to build muscle while on tirzepatide? Absolutely. With a calorie deficit, muscle gain is challenging but possible; in maintenance or surplus, many users gain lean tissue. The key is high protein (≥1.6 g/kg) + progressive overload.
Is tirzepatide hard on your body? It can be, especially GI tract, but serious adverse events are rare. Most side effects are mild-moderate and transient. Kidney/pancreatic risks exist but are uncommon.
Is tirzepatide stronger than Ozempic? Yes. In head-to-head trials (SURPASS), tirzepatide led to significantly greater A1c reduction and weight loss than semaglutide 1.0 mg.
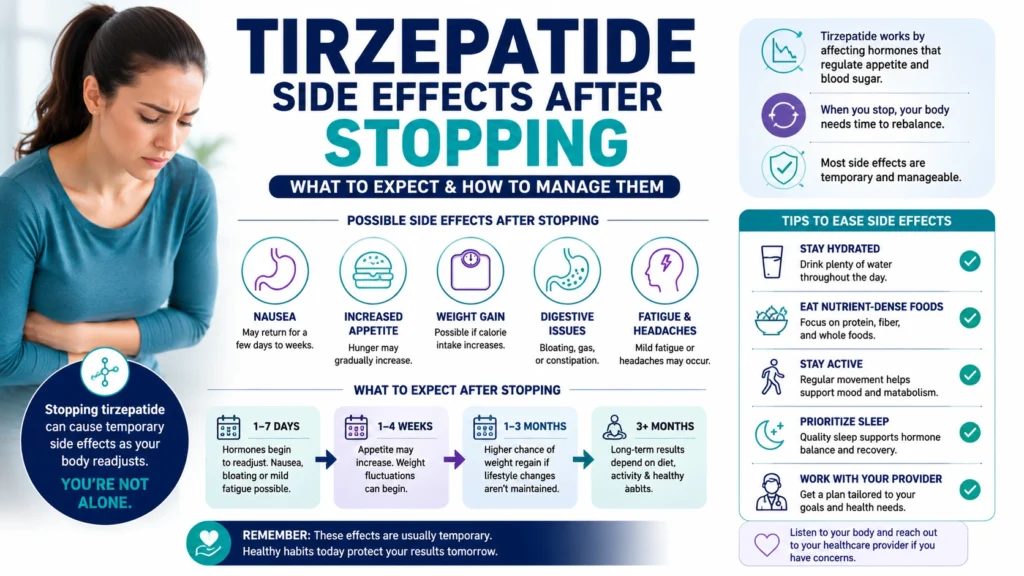
Side effects after stopping tirzepatide
- Rebound hunger – often the most noticeable; ghrelin increases
- Weight regain – rapid in first 4–8 weeks, tends to plateau
- Joint & muscle aches – some report arthralgia (see FAQ)
- GI rebound – constipation may shift to diarrhea, bloating
- Fatigue & mood shifts – due to changes in dopamine/GLP-1 signaling
Most effects diminish within 4–12 weeks, but metabolic rate may remain lower for months.
FAQ · 12 burning questions
Yes – reduces fat mass, spares lean mass with proper nutrition.
Yes, with high protein and resistance training, even in a deficit.
It can cause GI distress; serious risks are low but monitor pancreatitis.
Yes, in both A1c reduction and weight loss (SURPASS trials).
Yes, some report transient myalgia/arthralgia, usually mild.
No direct link; but GLP-1 may modulate inflammation; joint pain is rare.
Possibly immune modulation or dehydration; consult your doctor.
Reported in <1% of cases; often transient.
Yes, as above – prioritize protein and resistance.
No, muscle loss is reversible with training and nutrition.
Tirzepatide shows slightly better lean mass preservation in some studies.
Cost, GI side effects, rebound weight gain after stopping.
Pancreatitis, gallbladder disease, severe allergic reactions.
Using without obesity/diabetes increases risk of hypoglycemia, dehydration.
Dual GIP/GLP-1 may offset some GLP-1–mediated nausea.
Comparable; tirzepatide has more GI events at high doses, but often better tolerated overall.
Citations & references
SURMOUNT-1 & SURMOUNT-4 (NEJM 2022, 2023); SURPASS-2 (Lancet 2021); meta-analysis on GLP-1 receptor agonists and body composition (Obesity Reviews 2024).
Disclosure & disclaimer
This article contains affiliate links. If you purchase through the link, we may earn a small commission at no extra cost to you. All information is for educational purposes only and does not replace medical advice. Always consult your healthcare provider before starting or stopping any medication. Results vary.
PS. The affiliate link (track.revoffers.com) is sponsored and helps keep this resource free.
Medical disclaimer: Tirzepatide is a prescription drug. Do not stop or adjust dose without medical supervision. Withdrawal effects can include rapid weight regain, hyperglycemia, and GI distress.
written with care · 2026