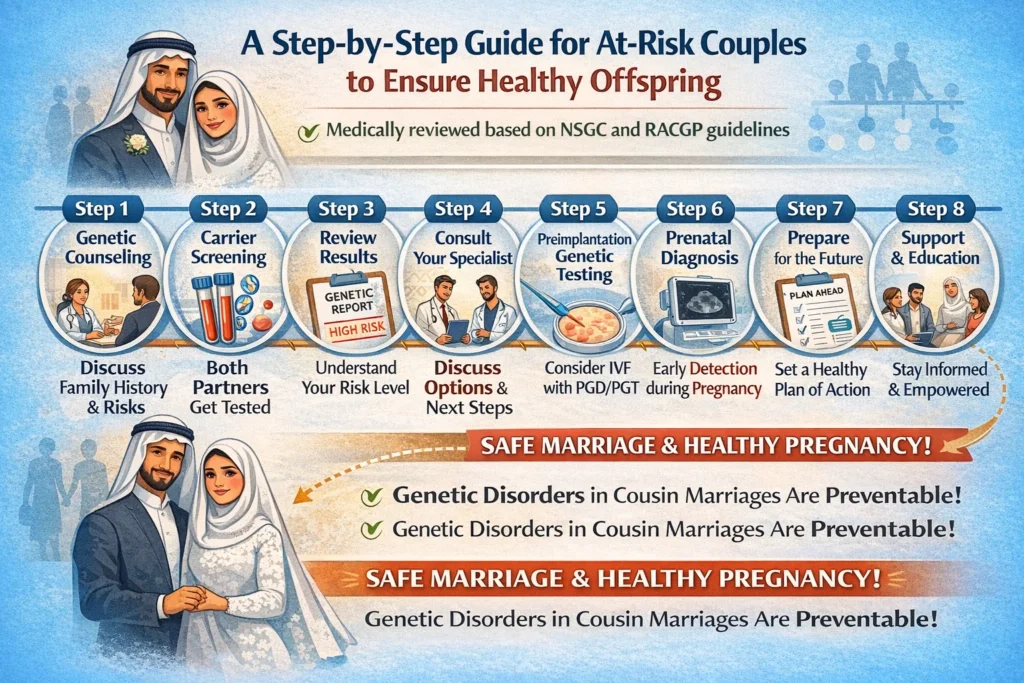
A Step-by-Step Guide for At-Risk Couples to Ensure Healthy Offspring
Medically reviewed based on NSGC and RACGP guidelines
For millions of couples worldwide, marriage between cousins is a deeply rooted cultural, religious, and familial tradition. In fact, consanguineous unions—defined as marriages between individuals related as second cousins or closer—account for approximately 10% of marriages globally, with higher concentrations in South Asia, the Middle East, and North Africa .
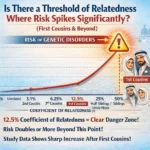
However, the biological reality is undeniable: when blood relatives have children together, the risk of autosomal recessive genetic disorders increases significantly. The closer the biological relationship, the higher the probability that both parents carry the same disease-causing gene variants—which means a 25% chance with every pregnancy that the child will inherit two copies of a faulty gene.
But here’s the empowering truth: genetic disorders in cousin marriages are largely preventable.
This article provides a clinical-grade, actionable checklist for consanguineous couples planning pregnancy. Based on recommendations from the National Society of Genetic Counselors (NSGC), the Royal Australian College of General Practitioners (RACGP) , and peer-reviewed research, this checklist will guide you through every stage—from preconception to postnatal care.
Understanding the Risk: Why Cousin Marriages Require Extra Caution
First, let’s clarify the actual risk. Many people overestimate or underestimate the dangers.
| Relationship | Shared DNA | Baseline Risk of Genetic Disorder |
|---|---|---|
| Unrelated parents | ~0% | 2–3% |
| First cousins | ~12.5% | 4–6% (approximately double) |
| Second cousins | ~3.125% | Slightly elevated |
A study of 66 consanguineous couples who underwent comprehensive genetic testing revealed that approximately 31% had identifiable genetic abnormalities, and another 17% had chromosomal polymorphic variations or variants of uncertain significance . These findings underscore why proactive screening is not fear-mongering—it’s responsible family planning.
The key takeaway: Most children born to cousins are healthy. However, the relative risk is doubled, which makes preconception genetic screening a medical priority rather than an optional extra.
The Checklist Approach: A Stage-by-Stage Prevention Plan
Stage 1: Preconception (Before Pregnancy)
Goal: Identify carrier status for recessive genetic disorders before conception occurs.
☐ Step 1: Comprehensive Three-Generation Family History
The NSGC consensus statement emphasizes that the single most important screening tool is a thorough medical family history covering at least three generations . This should include:
- Any previous children with known genetic conditions
- Unexplained infant deaths or stillbirths
- Family members with developmental delays, metabolic disorders, or congenital anomalies
- Known carrier status for conditions like thalassemia, cystic fibrosis, or spinal muscular atrophy (SMA)
Action item: Schedule a dedicated genetic counseling session before discontinuing contraception. Both partners must attend.
☐ Step 2: Preconception Expanded Carrier Screening (ECS)
According to RACGP guidelines, all couples planning pregnancy should be offered carrier screening, regardless of family history or ethnicity . For consanguineous couples, this is non-negotiable.
What to request from your provider:
- Basic panel: Cystic fibrosis, spinal muscular atrophy (SMA), fragile X syndrome
- Expanded panel: Up to several hundred recessive disorders (particularly those prevalent in your ethnic background)
- Hemoglobinopathy screening: Especially for those of Mediterranean, African, or Asian descent
The sequential screening approach:
- Screen one partner (usually the woman)
- If she is a carrier for any autosomal recessive condition, screen the other partner
- If both carry mutations in the same gene, genetic counseling is urgently indicated
Critical statistic: In one study, comprehensive genetic testing of consanguineous couples using exome sequencing identified shared carrier status for recessive disorders that would have been missed by standard panels .
☐ Step 3: Discuss Reproductive Options Before Pregnancy
If both partners are carriers for the same condition, you have several evidence-based options:
| Option | Description | Success Rate |
|---|---|---|
| Preimplantation Genetic Testing (PGT) | IVF with embryo screening for genetic disorders | 30–40% per cycle |
| Prenatal Diagnosis | CVS or amniocentesis during pregnancy | >99% accuracy |
| Gamete Donation | Using donor eggs or sperm | Varies |
| Adoption | Alternative parenting path | Varies |
Recommendation: Meet with a reproductive geneticist before pregnancy to understand these options fully. The NSGC emphasizes that providing preconception reproductive options is a primary goal of counseling .
Stage 2: Prenatal (During Pregnancy)
Goal: Detect potential fetal abnormalities early to enable informed decision-making and preparation.
☐ Step 4: First-Trimester Combined Screening
The NSGC recommends that consanguineous couples be offered maternal–fetal serum marker screening and high-resolution fetal ultrasonography during pregnancy .
Timeline:
- Weeks 10–13: Cell-free DNA screening (NIPT) for chromosomal conditions
- Weeks 11–14: Nuchal translucency ultrasound + serum PAPP-A and β-hCG
NIPT is now considered an acceptable first-line screening test for fetal chromosome abnormalities and is usually available from 10 weeks gestation .
☐ Step 5: Second-Trimester Detailed Anatomy Scan
At weeks 18–22, a high-resolution fetal ultrasound (sometimes called a “level II” ultrasound) should be performed. This is particularly important for consanguineous couples because many recessive disorders have structural manifestations visible on ultrasound.
What the sonographer will evaluate:
- Brain and spinal cord development
- Heart structure and function
- Abdominal wall and gastrointestinal tract
- Kidney and bladder formation
- Limb and skeletal development
☐ Step 6: Consider Diagnostic Testing if Indicated
If screening tests raise concerns, or if both parents are confirmed carriers of a recessive disorder, diagnostic testing may be recommended:
- Chorionic Villus Sampling (CVS): Weeks 10–13
- Amniocentesis: Weeks 15–20
These tests carry a small risk of miscarriage (approximately 1 in 500–1,000) but provide definitive diagnosis.
Stage 3: Postnatal (After Birth)
Goal: Early detection of treatable conditions to prevent lifelong disability.
☐ Step 7: Newborn Screening (Within 48 Hours)
The NSGC specifically recommends that newborns of consanguineous couples be screened for:
- Impaired hearing (newborn hearing screening)
- Treatable inborn errors of metabolism (heel prick blood test)
Why this matters: Many recessive metabolic disorders are treatable if caught early but cause irreversible brain damage or death if missed. Phenylketonuria (PKU), biotinidase deficiency, and maple syrup urine disease are classic examples.
☐ Step 8: Follow-Up Pediatric Genetics Consultation
If any newborn screening result is abnormal, or if the infant has physical findings suggestive of a genetic syndrome, request an immediate referral to a clinical geneticist or metabolic specialist.
Red flags requiring prompt evaluation:
- Hypotonia (floppy baby)
- Dysmorphic facial features
- Feeding difficulties or failure to thrive
- Seizures in the first weeks of life
- Jaundice that persists beyond two weeks
What the Experts Say: Official Recommendations
National Society of Genetic Counselors (NSGC)
The NSGC convened a Consanguinity Working Group with expertise in genetic counseling, medical genetics, biochemical genetics, genetic epidemiology, pediatrics, perinatology, and public health genetics. Their consensus statement includes these key points :
“Beyond a thorough medical family history with follow-up of significant findings, no additional preconception screening is recommended for consanguineous couples. Consanguineous couples should be offered similar genetic screening as suggested for any couple of their ethnic group.”
However, they emphasize that prenatal screening should be more comprehensive, including maternal–fetal serum markers and high-resolution fetal ultrasound.
Royal Australian College of General Practitioners (RACGP)
The RACGP guidelines state that all women/couples planning pregnancy should have a comprehensive family history recorded to identify relatives with heritable genetic disorders, as well as the presence of consanguinity .
UK National Health Service (NHS)
NHS England has published training modules about close relative marriage and genetic risk for midwives and health visitors, as well as guidance on how to submit data around consanguinity and pregnancy to the Maternity Services Dataset . The NHS is also piloting new models of care to improve equitable access to genetic services for consanguineous couples.
Addressing Cultural Sensitivity: A Critical Component
Genetic counselors and healthcare providers must approach consanguinity with cultural humility. The NSGC explicitly lists “respecting psychosocial and multicultural issues” as one of its four primary goals .
For couples from communities where cousin marriage is traditional:
- Understand that you are not being judged for your family choices
- Genetic counseling is about empowerment, not prohibition
- Many religious traditions (including Islam and some branches of Judaism and Christianity) permit cousin marriage while encouraging health screening
The NSGC emphasizes that healthcare providers must recognize that consanguineous partnerships have deep cultural, religious, and familial significance and should not be stigmatized in healthcare systems .
Frequently Asked Questions
Q1: Are all cousin marriages equally risky?
A: No. First cousins share approximately 12.5% of their DNA, while second cousins share about 3.125%. The risk decreases significantly with more distant relationships. The NSGC defines consanguinity for screening purposes as second cousins or closer .
Q2: If our families have no history of genetic disorders, do we still need screening?
A: Yes. Many recessive disorders appear “out of nowhere” in consanguineous families precisely because both parents carry the same mutation without knowing it. Family history is important, but carrier screening identifies risks that family history misses .
Q3: What if we are already pregnant?
A: It’s not too late. Proceed immediately to Stage 2 (Prenatal) of this checklist. High-resolution ultrasound and diagnostic testing (CVS or amniocentesis) can still identify many conditions.
Q4: How much does genetic carrier screening cost?
A: In the USA, expanded carrier screening typically costs $200–$500 out-of-pocket, though many insurance plans cover it. Some conditions (like cystic fibrosis, SMA, and fragile X) have MBS/insurance rebates in various countries. Always check with your provider and insurer.
Q5: Does a positive carrier result mean we shouldn’t have children?
A: Absolutely not. Being a carrier for a recessive disorder is extremely common—most people carry 2–5 recessive mutations without knowing it. If both partners carry the same condition, you have reproductive options (PGT, prenatal diagnosis, donor gametes) that allow you to have healthy children.
Q6: Should we test existing children?
A: If you already have children and are concerned about genetic risks, consult a genetic counselor. Testing may be recommended if specific symptoms are present, but routine screening of asymptomatic children is generally not indicated.
Summary Checklist: Quick Reference Card
Print this section and bring it to your healthcare provider.
Preconception (Before Pregnancy)
- Schedule genetic counseling appointment (both partners)
- Complete three-generation family history
- Undergo expanded carrier screening (blood or saliva)
- Discuss results with genetic counselor
- If both carriers for same condition → explore PGT or prenatal diagnosis options
Prenatal (During Pregnancy)
- First-trimester NIPT + nuchal translucency scan (weeks 10–13)
- High-resolution fetal anatomy ultrasound (weeks 18–22)
- Consider CVS or amniocentesis if indicated
Postnatal (After Birth)
- Complete newborn screening (heel prick + hearing test)
- Schedule pediatric follow-up within first week
- Request genetics referral for any abnormal findings
The Bottom Line
Preventing genetic disorders in cousin marriages is not about avoiding love or tradition—it’s about armed with information, you can make empowered decisions.
The checklist approach outlined above—preconception carrier screening, comprehensive prenatal monitoring, and prompt postnatal follow-up—can reduce the risk of having a child with a severe recessive genetic disorder from double the baseline risk to near-zero.
The NSGC, RACGP, and global genetics community all agree: consanguineous couples who undergo proper genetic screening have excellent outcomes. The key is starting the process before pregnancy, not after.
Don’t leave your child’s health to chance. Use this checklist, talk to a genetic counselor, and take control of your family’s genetic future.
Disclaimer: This information is for educational purposes only and is not a substitute for professional medical advice. Always consult with a licensed genetic counselor, obstetrician, or clinical geneticist for personalized recommendations based on your specific family history and genetic test results.