
For decades, the window into the health of a developing baby was limited. Expectant parents often faced a difficult choice: accept the limited accuracy of traditional screens or undergo invasive procedures like amniocentesis, which, while diagnostic, carried a small risk of miscarriage. That landscape has been fundamentally transformed by a remarkable discovery in maternal blood. This article explores what cell-free fetal DNA (cffDNA) is and why its analysis has become a cornerstone of modern prenatal care.
The Science: What Is Cell-Free Fetal DNA?
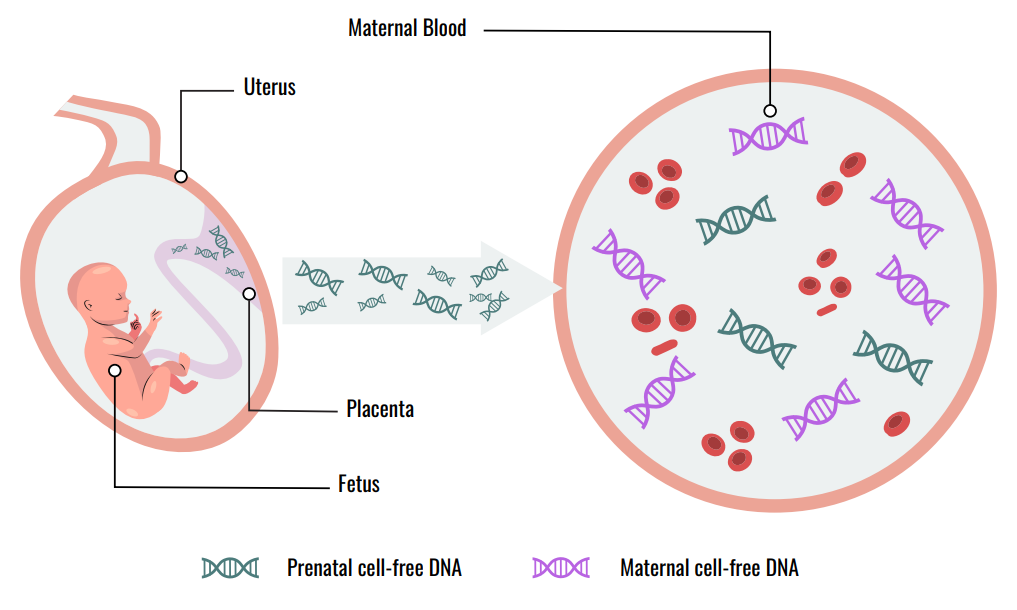
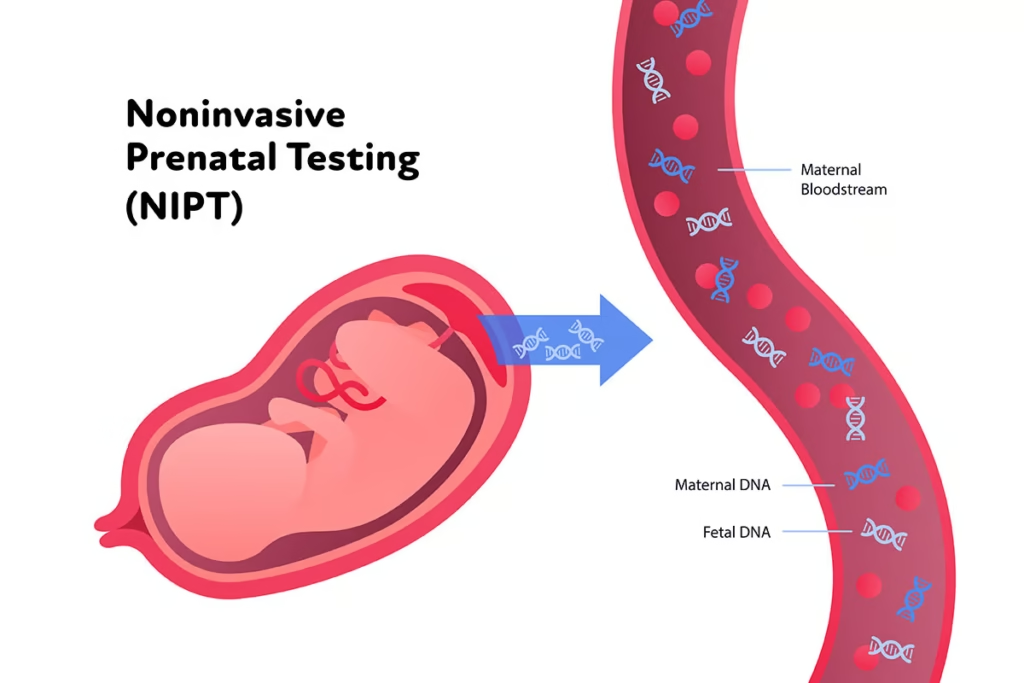
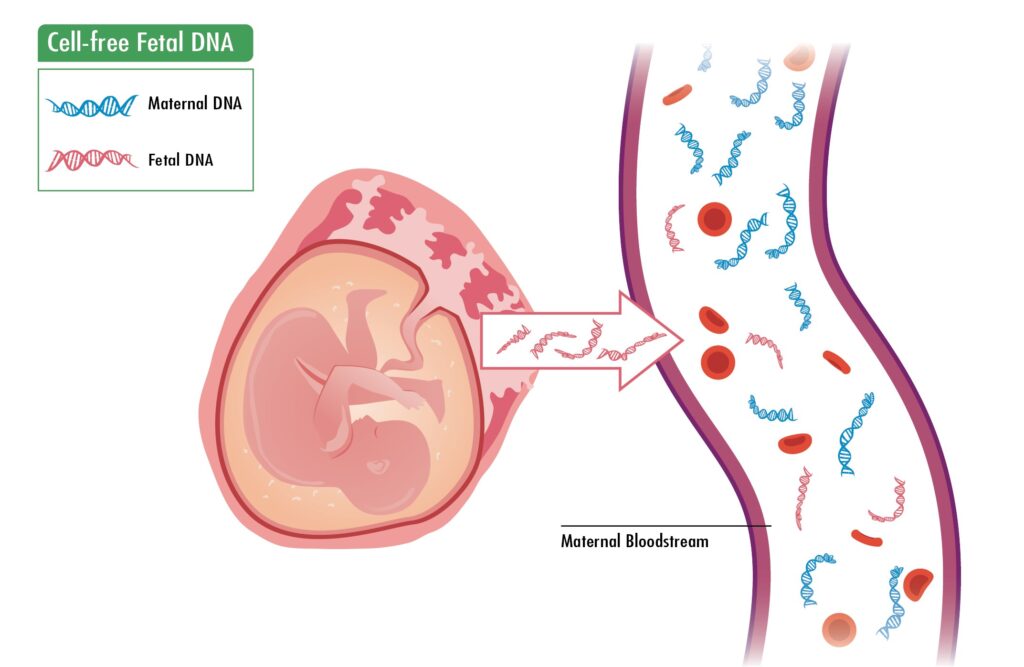
To understand this revolutionary test, one must first understand what it analyzes. Cell-free fetal DNA refers to small fragments of genetic material that circulate freely in the bloodstream of a pregnant woman. Contrary to initial assumptions, this DNA does not come directly from the fetus itself. Instead, it originates from the placenta . As placental cells (specifically, syncytiotrophoblasts) undergo their natural lifecycle, they break down and release tiny fragments of DNA into the maternal circulation .
This process begins very early in pregnancy. CffDNA can be detected in maternal plasma as early as five to six weeks of gestation . It is important to note that this fetal DNA is just a small piece of the genetic picture. The majority of cell-free DNA in a pregnant woman‘s blood—about 90%—comes from her own cells . The proportion of cffDNA in a sample is known as the “fetal fraction.” This fraction typically ranges from 10% to 20% during the first and second trimesters and is a critical factor for test accuracy . After the baby is born, cffDNA is rapidly cleared from the mother’s bloodstream within hours, making it specific to the ongoing pregnancy .
From Discovery to Clinical Application
The journey from scientific discovery to routine clinical tool has been swift. Following the initial identification of cffDNA in 1997, scientists realized they had found a potential “liquid biopsy” from the placenta .
The earliest clinical uses were highly specific. Because the fetal DNA is mixed with the mother‘s, initial applications focused on detecting genetic sequences that the mother did not possess. This made it relatively straightforward to test for paternally inherited traits, such as the presence of Y-chromosome sequences for fetal sex determination or the RHD gene in RhD-negative mothers to assess the risk of blood incompatibility .
The real paradigm shift occurred with the advent of next-generation sequencing (NGS) technologies. These advanced tools allowed scientists to count millions of DNA fragments with incredible precision. This was the breakthrough that enabled Non-Invasive Prenatal Testing (NIPT) for common chromosomal disorders .
Why Doctors Use It: Detecting Genetic Disorders
Today, the analysis of cffDNA is primarily used as a highly accurate screening tool. It is important to emphasize that NIPT is a screening test, not a diagnostic one. A “positive” result indicates an increased risk and must be confirmed with invasive diagnostic testing like chorionic villus sampling (CVS) or amniocentesis . So, why do doctors use it? The answer lies in its unparalleled performance and safety profile.
1. Gold-Standard Screening for Common Aneuploidies
The most established and widespread use of cffDNA analysis is for detecting fetal aneuploidies—conditions caused by missing or extra chromosomes. Major medical organizations, including the American College of Obstetricians and Gynecologists (ACOG), now recommend that cfDNA screening for common aneuploidies be made routinely available to all pregnant patients .
- Trisomy 21 (Down syndrome): NIPT demonstrates exceptional accuracy, with detection rates exceeding 99% .
- Trisomy 18 (Edwards syndrome) and Trisomy 13 (Patau syndrome): Detection rates are also very high, ranging from 90% to 99% .
Compared to traditional first-trimester screening (which measures biochemical markers and nuchal translucency), NIPT offers superior sensitivity and specificity, dramatically reducing the number of false positives and the consequent anxiety and need for unnecessary invasive procedures .
2. The Expanding Scope: Beyond the Common Three
The technology continues to evolve, and the applications for cffDNA are expanding into more complex areas .
- Sex Chromosome Aneuploidies (SCAs): NIPT can screen for conditions involving the sex chromosomes, such as Turner syndrome (monosomy X), Klinefelter syndrome (XXY), and triple X syndrome (XXX). However, the performance is more variable, with lower positive predictive values than for trisomy 21, and it is often offered as an optional screen requiring thorough pre-test counseling .
- Microdeletion Syndromes: Some expanded NIPT panels screen for conditions like 22q11.2 deletion syndrome (DiGeorge syndrome), which are caused by tiny missing pieces of a chromosome. The clinical use of these panels remains a topic of discussion due to the rarity of the conditions and lower predictive values. Professional guidelines currently do not recommend routine population screening for microdeletions .
- Monogenic Disorders: For families at high risk of passing on a specific single-gene disorder (like achondroplasia or cystic fibrosis), cffDNA analysis can be used for definitive diagnosis (NIPD), particularly for paternally inherited or de novo mutations .
3. Beyond Genetics: A Window into Placental Health
Emerging research suggests that cffDNA levels themselves may serve as a biomarker for placental health. Abnormal levels—either too high or too low—have been associated with complications such as preeclampsia and fetal growth restriction (FGR) , offering a potential early warning system for obstetric complications that extend far beyond genetic disorders .
The Importance of Professional Guidance
While cffDNA testing is a powerful tool, it is not without complexities. Factors like maternal weight, gestational age, and multiple pregnancies (twins, etc.) can affect the fetal fraction and test performance . Results can also be complicated by “confined placental mosaicism,” where the placenta’s genetic makeup differs from that of the fetus, leading to a false-positive screen .
Therefore, pre- and post-test genetic counseling is essential. Patients must understand the difference between screening and diagnosis, the conditions being tested for, and the implications of the results. A positive NIPT result always requires confirmation with a diagnostic test, and a negative result does not guarantee a baby without any genetic condition .
Conclusion: A Paradigm Shift in Prenatal Care
The discovery and analysis of cell-free fetal DNA has undoubtedly been a paradigm shift in prenatal medicine . It has transformed the experience of pregnancy for millions by offering a safe, early, and highly accurate window into fetal health. By dramatically reducing the need for invasive procedures and providing clearer answers earlier, cffDNA analysis empowers clinicians and expectant parents with better information for decision-making. As technology advances toward even more comprehensive genome-wide analysis, the role of this remarkable tool in fetal medicine will only continue to grow, solidifying its place as one of the most significant breakthroughs in modern obstetrics