
1. Tumor Shrinkage on Imaging Scans (The Gold Standard)
The most definitive sign is a reduction in tumor size or complete disappearance of tumors, as seen on CT, PET, or MRI scans.
- Timing: Unlike chemotherapy, which often kills cancer cells quickly, immunotherapy activates the immune system, which then attacks the tumor. This process can take 2 to 3 months or longer. Scans are typically done every 9–12 weeks.
- Pseudoprogression: A unique phenomenon where the tumor initially appears larger or new lesions appear because immune cells (T-cells) have flooded the tumor site, causing inflammation and swelling. After a few more weeks, the tumor then shrinks. True progression vs. pseudoprogression is distinguished by a follow-up scan (usually 4–8 weeks later) or by a PET scan showing metabolic activity drop.
2. Stabilization of Disease (No New Growth)
Even if the tumor doesn’t shrink, stable disease for an extended period (e.g., 6+ months) is a positive sign. Cancer that stops growing or spreading indicates the immune system has put a “blockade” around it.
3. Improvement in Cancer-Related Symptoms
As the immune system attacks cancer, systemic symptoms often improve. Examples include:
- Pain reduction: Less bone or organ pain due to shrinking tumors.
- Energy increase: Resolution of cancer-related fatigue (though immune-related fatigue can occur).
- Weight gain/stabilization: Reversal of cachexia (wasting syndrome).
- Breathing improvement: For lung cancer patients, less shortness of breath.
- Appetite return: Normalization of eating patterns.
4. Blood-Based Markers
Several blood tests can hint at a response:
- Circulating Tumor DNA (ctDNA) drop: A liquid biopsy showing a significant decrease in tumor DNA fragments in the blood often precedes radiographic response by weeks.
- Normalization of tumor markers: For cancers like melanoma (LDH), ovarian (CA-125), or prostate (PSA), a sustained drop in these markers is encouraging.
- Complete blood count (CBC): Improvement in anemia or white blood cell counts if the bone marrow was involved.
- New onset of immune-related blood changes: Mild lymphocytosis (increase in lymphocytes) early in treatment sometimes correlates with better outcomes.
5. Clinical Signs of Immune Activation (Often Paradoxical)
Ironically, the side effects of immunotherapy (immune-related adverse events, or irAEs) can be signs that the immune system is revved up and attacking the cancer. However, not all patients with side effects respond, and not all responders have side effects.
Common irAEs that may correlate with response:
- Skin rash (maculopapular or vitiligo-like depigmentation – especially in melanoma).
- Diarrhea/colitis (mild to moderate).
- Thyroiditis (leading to hyper- then hypothyroidism).
- Arthralgia/myositis (joint/muscle inflammation).
- Pneumonitis (lung inflammation – requires careful monitoring).
Note: Severe irAEs require treatment with steroids, which can dampen the anti-cancer effect if overused.
6. Durable Response After Treatment Ends
One hallmark of immunotherapy is memory T-cell response. A patient may stop treatment after 1–2 years (if stable/responding) and remain cancer-free for years. This is a late sign that immunotherapy has “trained” the immune system to remember the cancer.
7. Pathologic Complete Response (pCR)
If a patient undergoes a biopsy or surgery after neoadjuvant immunotherapy (treatment before surgery), the pathologist may find no viable cancer cells in the tissue sample. This is a definitive sign of a deep response.
Important Caveats & What Is NOT a Sign
| Misleading Sign | Explanation |
|---|---|
| Feeling worse initially | Immune activation can cause flu-like symptoms (fever, fatigue, muscle aches) for days after infusion. This is not failure. |
| New “tumor” on first scan | Could be pseudoprogression – requires repeat scan in 4-8 weeks. |
| Sudden severe side effects | May require immune suppression; does not automatically mean better cancer response. |
| No side effects | Many long-term responders have zero irAEs. |
Summary Table: Early vs. Late Signs of Response
| Timeline | Signs |
|---|---|
| Weeks 1–4 | Mild fatigue, low-grade fever, rash; no scan changes. |
| Weeks 8–12 | Symptom improvement (less pain, better appetite); possible pseudoprogression on first scan. |
| Months 3–6 | Objective tumor shrinkage or stable disease on repeat scan; drop in ctDNA/tumor markers. |
| Months 12+ | Continued response off treatment; pathologic complete response if biopsied. |
When to Suspect It Is NOT Working
- Progressive disease on two consecutive scans (4–8 weeks apart) with growing or new lesions.
- Worsening performance status (bedridden, severe weight loss) without another cause.
- Rising tumor markers over 2–3 consecutive measurements.
Final Clinical Pearl
Do not stop immunotherapy based on the first scan alone. Always confirm progression with a second scan or biopsy if pseudoprogression is suspected. Many durable responses have been seen in patients whose tumors initially “lit up” or grew slightly before shrinking. Always discuss results with your oncologist, who can use tools like iRECIST (immune-specific response criteria) to interpret findings correctly.
give examples of immunotherapy
Certainly. Based on the previous discussion about how to tell if immunotherapy is working, here are the major examples of immunotherapy used in cancer treatment today. They are categorized by how they work.
Immunotherapy is not a single drug but a class of therapies that all aim to use the immune system to fight cancer. The most common and successful examples are immune checkpoint inhibitors, but there are several other types.
1. Immune Checkpoint Inhibitors (Most Common)
These drugs block “brakes” on immune cells (T-cells), allowing them to attack cancer. They are often called “-mab” drugs.
| Drug Name (Brand) | Target | Common Cancers Treated |
|---|---|---|
| Pembrolizumab (Keytruda) | PD-1 | Melanoma, lung cancer, head/neck cancer, bladder cancer, Hodgkin lymphoma, triple-negative breast cancer, MSI-high solid tumors. |
| Nivolumab (Opdivo) | PD-1 | Melanoma, lung cancer, kidney cancer, colon cancer, liver cancer, Hodgkin lymphoma. |
| Cemiplimab (Libtayo) | PD-1 | Cutaneous squamous cell carcinoma, basal cell carcinoma, lung cancer. |
| Dostarlimab (Jemperli) | PD-1 | Endometrial cancer, MSI-high solid tumors. |
| Atezolizumab (Tecentriq) | PD-L1 | Lung cancer, bladder cancer, triple-negative breast cancer, liver cancer. |
| Avelumab (Bavencio) | PD-L1 | Merkel cell carcinoma, bladder cancer, kidney cancer. |
| Durvalumab (Imfinzi) | PD-L1 | Lung cancer (after chemoradiation), bladder cancer. |
| Ipilimumab (Yervoy) | CTLA-4 | Melanoma, kidney cancer, colon cancer (often combined with nivolumab). |
| Tremelimumab (Imjudo) | CTLA-4 | Liver cancer (combined with durvalumab). |
Note: MSI-high stands for “microsatellite instability-high,” a biomarker that predicts a strong response to PD-1 inhibitors.
2. CAR T-Cell Therapy (Cell-Based Immunotherapy)
This is a personalized treatment where a patient’s own T-cells are removed, genetically engineered to recognize cancer, multiplied, and infused back into the patient.
| Drug Name (Brand) | Target | Common Cancers Treated |
|---|---|---|
| Tisagenlecleucel (Kymriah) | CD19 | B-cell acute lymphoblastic leukemia (ALL) in children/young adults, diffuse large B-cell lymphoma (DLBCL). |
| Axicabtagene ciloleucel (Yescarta) | CD19 | DLBCL, primary mediastinal B-cell lymphoma, follicular lymphoma. |
| Brexucabtagene autoleucel (Tecartus) | CD19 | Mantle cell lymphoma, B-ALL. |
| Lisocabtagene maraleucel (Breyanzi) | CD19 | DLBCL, high-grade B-cell lymphoma. |
| Idecabtagene vicleucel (Abecma) | BCMA | Multiple myeloma. |
| Ciltacabtagene autoleucel (Carvykti) | BCMA | Multiple myeloma. |
3. Bispecific T-Cell Engagers (BiTEs)
These drugs are antibodies that bind to both a cancer cell and a T-cell, physically bringing them together so the T-cell can kill the cancer.
| Drug Name (Brand) | Targets (Cancer / T-cell) | Common Cancers Treated |
|---|---|---|
| Blinatumomab (Blincyto) | CD19 (cancer) / CD3 (T-cell) | B-cell ALL. |
| Teclistamab (Tecvayli) | BCMA (cancer) / CD3 (T-cell) | Multiple myeloma. |
| Mosunetuzumab (Lunsumio) | CD20 (cancer) / CD3 (T-cell) | Follicular lymphoma. |
| Glofitamab (Columvi) | CD20 (cancer) / CD3 (T-cell) | DLBCL. |
4. Cancer Vaccines (Therapeutic)
Unlike preventive vaccines (e.g., HPV vaccine), these treat existing cancer by training the immune system to attack tumor-specific antigens.
| Name | Type | Cancers Treated |
|---|---|---|
| Sipuleucel-T (Provenge) | Dendritic cell vaccine (patient’s own immune cells exposed to a protein) | Metastatic prostate cancer (hormone-refractory). |
| Talimogene laherparepvec (T-VEC / Imlygic) | Oncolytic virus vaccine (modified herpes virus injected into tumors) | Advanced melanoma (injectable lesions). |
5. Immune System Modulators (Cytokines & Adjuvants)
These are older forms of immunotherapy that broadly stimulate or suppress the immune system.
| Drug Name | Type | Cancers Treated (historically or currently) |
|---|---|---|
| Interleukin-2 (IL-2, Proleukin) | Cytokine (stimulates T-cell growth) | Metastatic melanoma, kidney cancer (now less common due to toxicity). |
| Interferon-alpha (Intron A) | Cytokine (activates immune cells) | Melanoma, hairy cell leukemia, Kaposi sarcoma. |
| Bacillus Calmette-Guérin (BCG) | Live attenuated bacteria (instilled into bladder) | Non-muscle invasive bladder cancer (gold standard for decades). |
6. Monoclonal Antibodies (for Immune Modulation)
While many antibodies are checkpoint inhibitors, some work by tagging cancer cells for destruction (antibody-dependent cellular cytotoxicity, or ADCC).
| Drug Name (Brand) | Target | Mechanism | Cancers |
|---|---|---|---|
| Rituximab (Rituxan) | CD20 (on B-cells) | Tags B-cell lymphomas for immune destruction | Non-Hodgkin lymphoma, CLL. |
| Trastuzumab (Herceptin) | HER2 (on breast/gastric cancer) | Tags HER2+ cells | HER2+ breast cancer, gastric cancer. |
| Cetuximab (Erbitux) | EGFR | Tags EGFR+ cells | Colon cancer, head/neck cancer. |
Note: Rituximab and trastuzumab are often classified as “targeted therapy” but work partly via the immune system (ADCC), so they sit at the intersection.
Summary by Cancer Type (Common Examples)
| Cancer Type | Common Immunotherapy Examples |
|---|---|
| Melanoma | Pembrolizumab, nivolumab, ipilimumab, T-VEC, IL-2 |
| Non-small cell lung cancer | Pembrolizumab, nivolumab, atezolizumab, durvalumab |
| Bladder cancer | Atezolizumab, pembrolizumab, nivolumab, BCG (for early stage) |
| Hodgkin lymphoma | Pembrolizumab, nivolumab, brentuximab vedotin (antibody-drug conjugate) |
| Multiple myeloma | Daratumumab (anti-CD38 antibody), teclistamab, ide-cel CAR T |
| Prostate cancer | Sipuleucel-T (Provenge) |
| Colorectal cancer (MSI-high) | Pembrolizumab, nivolumab |
| Breast cancer (triple-negative) | Atezolizumab, pembrolizumab |
If you are looking for a specific type of cancer not listed, let me know, and I can provide the relevant immunotherapy examples.
keytruda immunotherapy
Read 10 web pages
Here is a detailed overview of Keytruda (pembrolizumab), one of the most widely used immunotherapy drugs for cancer treatment. This information builds on our previous discussions about how immunotherapy works and the signs that it is effective.
What Is Keytruda?
Keytruda is a brand name for pembrolizumab, a humanized monoclonal antibody that belongs to a class of drugs called immune checkpoint inhibitors. It is a type of immunotherapy that works by helping your immune system recognize and attack cancer cells.
Mechanism of Action
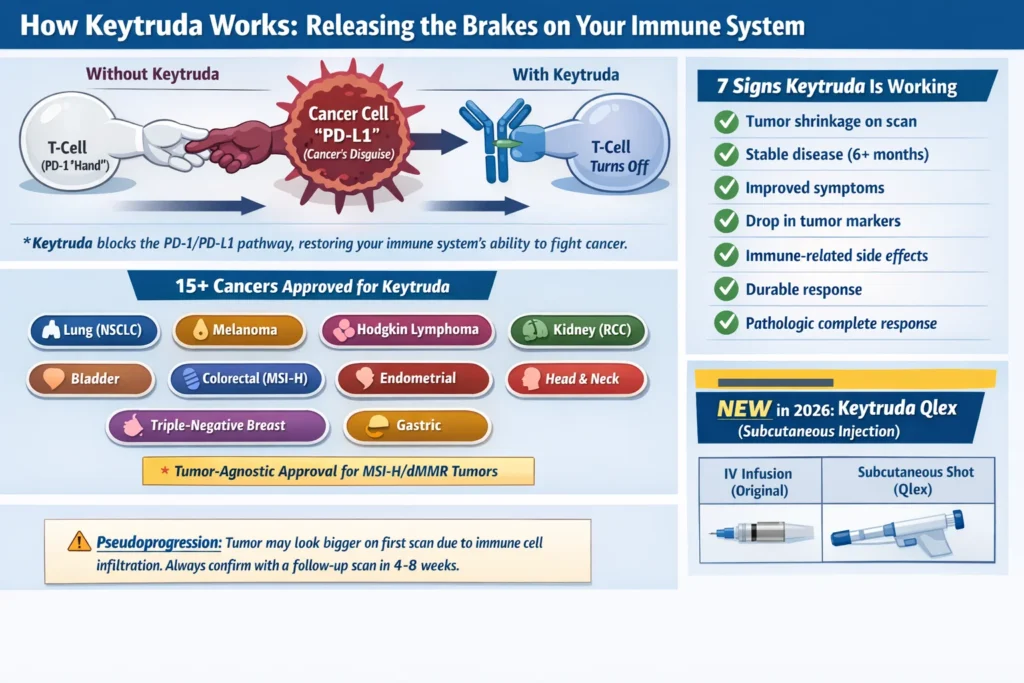
Keytruda works by blocking a protein called PD-1 (programmed cell death protein-1) found on the surface of immune cells called T-cells.
Here is how it works in simple terms:
- Normal Immune Function: T-cells are designed to find and destroy abnormal cells, including cancer cells.
- Cancer’s Evasion Tactic: Some cancers produce proteins called PD-L1 and PD-L2, which act like “handshakes” with the PD-1 receptor on T-cells. This interaction essentially turns off the T-cell, preventing it from attacking the cancer.
- How Keytruda Helps: Keytruda binds to the PD-1 receptor and blocks this “off switch.” By blocking the interaction, it restores the T-cell’s ability to recognize and fight the cancer cells.
Keytruda can be used alone (as monotherapy) or in combination with other cancer treatments like chemotherapy or other targeted therapies.
What Cancers Does Keytruda Treat?
Keytruda has been approved to treat a very wide range of cancers, making it one of the most versatile immunotherapies available. It is often used for advanced (metastatic) cancers or as an adjuvant therapy (after initial treatment like surgery) to lower the risk of cancer returning.
Here are some of the main cancer types Keytruda is approved for:
This is not a complete list, but it shows the broad range of cancers Keytruda can treat.
How Is Keytruda Given?
Keytruda is available in two forms: an intravenous (IV) infusion and a newer subcutaneous (under the skin) injection.
1. Intravenous (IV) Infusion (Original Form)
The traditional way to receive Keytruda is through an IV drip, which typically takes about 30 minutes.
2. Subcutaneous Injection: Keytruda Qlex
In late 2025, the FDA approved Keytruda Qlex, a new form of pembrolizumab that is given as a quick shot under the skin (subcutaneously).
- Administration: The injection is given by a healthcare provider into the thigh or abdomen and takes only 1 to 2 minutes.
- Dosing: Two convenient dosing options are available:
- Efficacy: Clinical trials showed that Keytruda Qlex is just as effective and safe as the IV version. In a study of 377 patients with advanced lung cancer, the response rate was 45% for the subcutaneous shot and 42% for the IV infusion.
This new option can be a major benefit for patients who have difficulty with IV access or want shorter clinic visits.
What Are the Side Effects of Keytruda?
Because Keytruda works by activating your immune system, it can cause your immune cells to attack not only cancer cells but also normal, healthy tissues. These are called immune-related adverse events (irAEs).
Common Side Effects
These are mild to moderate and often manageable. They include:
- Fatigue
- Muscle or joint pain
- Rash and itching (pruritus)
- Diarrhea
- Nausea
- Decreased appetite
- Cough and shortness of breath
- Hypothyroidism (underactive thyroid)
- Fever
Serious Immune-Related Side Effects (Less Common but Require Urgent Attention)
In some people, the immune system can attack specific organs, leading to serious inflammation that needs immediate medical treatment. These can include:
Important: If you experience any new or worsening symptoms while on Keytruda, contact your oncology team immediately. Early recognition and management of these side effects are critical.
How Do You Know If Keytruda Is Working?
As we discussed in detail previously, signs that Keytruda (or any immunotherapy) is working include:
- Tumor shrinkage or stabilization on follow-up CT, PET, or MRI scans (typically done every 9-12 weeks).
- Improvement in cancer-related symptoms such as less pain, increased energy, better appetite, and weight stabilization.
- Durable response after treatment ends, where the cancer remains in control for months or years.
- Pseudoprogression: A unique phenomenon where the tumor appears larger on the first scan due to immune cell infiltration before shrinking later. Always confirm progression with a follow-up scan.
Comparison: Keytruda (IV) vs. Keytruda Qlex (Subcutaneous)
Summary
Keytruda (pembrolizumab) is a powerful immunotherapy that has revolutionized cancer treatment for many types of cancer. It works by blocking the PD-1 pathway, allowing your immune system to attack cancer cells more effectively. With the recent approval of Keytruda Qlex, treatment is becoming more convenient with a quick, under-the-skin injection. While it can cause immune-related side effects, including rare but serious conditions like adrenal insufficiency, these are generally manageable with prompt medical care. Always discuss the potential benefits and risks with your oncologist based on your specific cancer type and overall health.

{kind=link}