A Public Health Emergency Declared
On May 17, 2026, the World Health Organization (WHO) declared the current Ebola outbreak 2026 a Public Health Emergency of International Concern (PHEIC) . The declaration came after more than 300 suspected cases and 88 deaths were reported across the Democratic Republic of the Congo (DRC) and neighboring Uganda.
This marks the 17th Ebola outbreak in DRC since the virus was first discovered near the Ebola River in 1976. But this time, the situation is different — and more concerning.
The Ebola virus disease outbreak is caused by the Bundibugyo strain, a rarer species of the virus for which no licensed vaccine or specific antiviral treatment exists.
“This outbreak does not meet the criteria of a pandemic emergency like COVID-19,” the WHO stated on X (formerly Twitter). “We advise against the closure of international borders.”
However, the agency emphasized that the event is serious, there is a risk of international spread, and it requires a coordinated international response.
Key Facts About the Current Ebola Outbreak 2026
| Fact | Detail |
|---|---|
| Declared | May 17, 2026 (PHEIC status) |
| Location | Ituri Province, DRC (epicenter) + spread to Uganda and Kinshasa |
| Suspected Cases | 336+ |
| Confirmed Deaths | 88 |
| Viral Strain | Bundibugyo ebolavirus |
| Vaccine Availability | ❌ None for this strain |
| Case Fatality Rate | 30-50% (historical) |
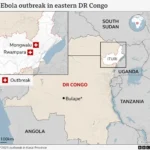
Where Is the Congo Ebola Outbreak Spreading?
The Congo Ebola outbreak began in rural areas of Ituri Province, eastern DRC. However, recent developments have raised global alarm:
1. Spread to Kinshasa (Capital City)
A laboratory-confirmed case has been reported in Kinshasa, the capital of DRC, which is approximately 1,000 kilometers (620 miles) from the outbreak’s epicenter in Ituri. The patient had traveled from Ituri to Kinshasa before becoming symptomatic.
This is a critical development because Kinshasa is a densely populated megacity with over 15 million residents and an international airport connecting to multiple continents.
2. Spread to Uganda
Two confirmed imported cases have been reported in Uganda, including one in the capital city of Kampala. Uganda shares a porous border with DRC, and cross-border trade and family movements are common.
3. Suspected Cases in North Kivu
Suspected cases have also been reported in North Kivu province — one of Congo’s most populous regions, bordering Ituri. North Kivu has experienced significant civil conflict and population displacement, making outbreak containment extremely challenging.
4. Risk to Neighboring Countries
The WHO has assessed the regional risk as “high,” with South Sudan, Rwanda, and Burundi considered vulnerable due to:
- Population movement across borders
- Limited healthcare infrastructure
- Ongoing humanitarian crises
Why This Ebola Virus Disease Outbreak Is Different
No Vaccine Available
Previous major Ebola outbreaks — including the 2014-2016 West Africa epidemic and the 2018-2020 DRC outbreak — were caused by the Zaire ebolavirus. For that strain, two licensed vaccines exist:
- rVSV-ZEBOV (Ervebo®) – single dose
- Ad26.ZEBOV + MVA-BN-Filo – two-dose regimen
However, the current Ebola outbreak 2026 is caused by the Bundibugyo virus. According to DRC Health Minister Samuel-Roger Kamba, this strain has “no vaccine and no specific treatment” and carries “a very high lethality rate which can reach 50 percent.”
High Fatality Despite Modern Medicine
Even with modern supportive care, the Bundibugyo strain historically kills between 30% and 50% of those infected. Without treatment — which is often unavailable in remote outbreak zones — the fatality rate can be even higher.
Urban Transmission Risk
The confirmation of a case in Kinshasa (a city of 15+ million) and spread to Kampala, Uganda (1.5+ million) significantly raises the risk of rapid, uncontrolled transmission. Urban environments feature:
- High population density
- Overcrowded public transport
- Limited access to clean water and sanitation in slum areas
- Informal healthcare providers who may not follow infection control protocols
How Does Ebola Spread?
Understanding transmission is critical for prevention. The Ebola virus disease outbreak spreads through:
Direct Contact With Bodily Fluids
- Blood
- Vomit
- Diarrhea
- Saliva
- Sweat
- Urine
- Breast milk
- Semen (remains infectious for months after recovery)
Contaminated Surfaces (Fomites)
- Needles and syringes
- Bedding and clothing
- Medical equipment
- Hospital surfaces
Animal-to-Human Transmission
- Fruit bats (natural reservoir)
- Chimpanzees and gorillas
- Forest antelope (bushmeat)
Important: Not Airborne
Unlike COVID-19 or influenza, Ebola does not spread through casual airborne transmission in normal daily interactions. You cannot catch it by walking past an infected person.
Symptoms of the Ebola Virus Disease Outbreak
Symptoms typically appear 2 to 21 days after exposure. The average incubation period is 8–10 days.
Early Symptoms
- Sudden fever (≥38°C / 100.4°F)
- Severe fatigue and weakness
- Muscle pain
- Headache
- Sore throat
Advanced Symptoms
- Vomiting (often severe)
- Watery diarrhea
- Rash (red, non-itchy)
- Internal and external bleeding (gums, nose, injection sites)
- Organ failure (liver, kidneys)
- Shock
⚠️ A person is not contagious until symptoms begin. Once symptoms appear, the infected individual becomes increasingly infectious as the illness progresses.
WHO and Global Response
PHEIC Declaration
The WHO’s emergency declaration (PHEIC) is designed to spur donor agencies and countries into action. By the WHO’s standards, it indicates:
- The event is serious
- There is a risk of international spread
- A coordinated international response is required
What the WHO Is Doing
- Deploying rapid response teams to Ituri and Kinshasa
- Supporting contact tracing (identifying and monitoring everyone exposed)
- Coordinating laboratory testing
- Advising against border closures (which can drive outbreaks underground)
- Mobilizing funding for the response
Challenges to Response
The global response to previous PHEIC declarations has been mixed. In 2024, when the WHO declared mpox outbreaks in Congo and elsewhere in Africa a global emergency, experts noted that the declaration “did little to get supplies like diagnostic tests, medicines and vaccines to affected countries quickly.”
Similar challenges may arise with the current Ebola outbreak 2026:
- No vaccine available for the Bundibugyo strain → cannot use ring vaccination
- Conflict zones in Ituri and North Kivu prevent responders from reaching communities
- Limited funding for global health emergencies (donor fatigue)
- Weak healthcare infrastructure in affected regions
What Travelers Need to Know
If You Plan to Travel to DRC or Uganda
| Do This | Avoid This |
|---|---|
| Monitor WHO and CDC updates daily | Non-essential travel to Ituri Province (Level 4 advisory) |
| Practice strict hand hygiene | Contact with sick people or corpses |
| Avoid healthcare facilities unless necessary | Eating bushmeat or handling bats/primates |
| Isolate and call ahead if you develop symptoms | Walking into a clinic unannounced |
After Returning from Affected Areas
- Monitor your health for 21 days
- If you develop fever, fatigue, vomiting, or bleeding:
- Isolate immediately
- Call your doctor or local health department BEFORE visiting
- Report your travel history clearly
Will This Become Another Pandemic?
The WHO has explicitly stated that the current Ebola outbreak 2026 does not meet the criteria of a pandemic emergency like COVID-19. Ebola is significantly less transmissible than respiratory viruses like influenza or SARS-CoV-2.
Key differences from COVID-19:
| Factor | Ebola | COVID-19 |
|---|---|---|
| Primary transmission | Direct contact with bodily fluids | Airborne (respiratory droplets/aerosols) |
| Infectious before symptoms | No | Yes (pre-symptomatic spread) |
| Asymptomatic spread | Very rare | Common |
| R0 (basic reproduction number) | 1.5–2.5 | 2.5–7+ (variants) |
However, the Congo Ebola outbreak remains a serious regional threat. If it spreads further into major urban centers or across multiple borders without a vaccine, it could overwhelm healthcare systems in some of the world’s most vulnerable countries.
Conclusion
The current Ebola outbreak 2026 — declared a Public Health Emergency of International Concern on May 17, 2026 — represents a serious test of global health preparedness. The Congo Ebola outbreak has already spread from rural Ituri Province to the capital city of Kinshasa (1,000 km away) and into neighboring Uganda.
Unlike previous Ebola crises, this Ebola virus disease outbreak is caused by the Bundibugyo strain, for which there is no licensed vaccine or specific treatment. This makes traditional public health measures — isolation, contact tracing, safe burials, and infection control — more critical than ever.
For most people outside Central Africa, the risk remains very low. But for the people of eastern DRC and their neighbors, this is a genuine emergency requiring urgent international support.
The world has learned much since the catastrophic 2014 West Africa Ebola epidemic. But as the 2026 outbreak shows, Ebola remains a formidable foe — one that demands respect, resources, and rapid action.
📚 Sources & Trusted Resources
- World Health Organization (WHO): www.who.int
- U.S. CDC Ebola Page: www.cdc.gov/vhf/ebola
- Africa CDC: africacdc.org
- DRC Ministry of Health: Follow local announcements
Last updated: May 18, 2026 | Based on WHO PHEIC declaration of May 17, 2026