
A special expert report on the 2026 Bundibugyo virus outbreak
In mid-May 2026, the World Health Organization (WHO) declared the Ebola outbreak in the Democratic Republic of the Congo (DRC) a Public Health Emergency of International Concern (PHEIC). This decision has left many people around the world asking the same question: How worried should I actually be? for Ebola Outbreak in DR Congo?
The short answer is nuanced. For most people outside Central Africa, the risk remains very low. However, for the region itself, and for several specific reasons that make this outbreak unique, the situation is genuinely concerning—not just for the DRC, but for its neighbors as well.
- Not a substitute for professional medical care – These guidelines are general and not a replacement for direct consultation with a healthcare provider.
- Situation-dependent advice – Outbreak conditions, viral strains (Bundibugyo virus), and local infrastructure vary. Always follow local health authorities.
- No doctor-patient relationship – Viewing this content does not create a medical relationship with the publisher.
- Emergency situations – If symptoms + exposure risk exist, isolate immediately and call your local Ebola hotline or emergency number before visiting any facility.
- No guarantee of accuracy – Medical knowledge about Ebola evolves rapidly. This may not reflect the most current recommendations.
- Liability waiver – The creators assume no liability for any injury, loss, or damage arising from reliance on this information.
- Bundibugyo strain limitation – No licensed vaccine exists for the current strain; some precautions are adapted from general Ebola protocols.
📞 Emergency & Trusted Resources
🌍 WHO: who.int | 🇺🇸 CDC: cdc.gov | 🌍 Africa CDC: africacdc.org
If in DRC or Uganda: Call your local Ministry of Health Ebola hotline before traveling to any clinic.
Here is a breakdown of why global health authorities are on high alert, and what this means for you.
The Core of the Concern: A “Different” Type of Ebola
Most people have heard of the devastating 2014-2016 West Africa epidemic, which was caused by the Zaire ebolavirus. The current outbreak is different. It is caused by the Bundibugyo virus, a rarer species of Ebola.
This distinction is critical for two reasons:
1. No Vaccine or Specific Treatment
Unlike the Zaire strain (which has two licensed vaccines), there is currently no licensed vaccine or specific antiviral treatment for the Bundibugyo virus. DRC Health Minister Roger Kamba stated bluntly that this strain has “no vaccine and no specific treatment” and carries “a very high lethality rate which can reach 50 percent”.
2. It is Still Deadly
While slightly less lethal than Zaire (which kills 60-90% of those infected), the Bundibugyo strain still has a historical case fatality rate between 30% and 50%. This means that without proper medical care, up to half of those infected may die.
Because there is no vaccine, health officials cannot use “ring vaccination” (the strategy that successfully contained previous outbreaks). They must rely entirely on traditional public health measures: isolating patients, tracing contacts, and safe burials.
Why the Numbers Are Worrying
As of mid-May 2026, the reported figures are climbing rapidly, and authorities suspect the true numbers are much higher.
The “Iceberg” Warning: The WHO has warned that there are “significant uncertainties” regarding the true number of infected persons. The high positivity rate of initial samples and the confirmation of cases in two countries suggests this outbreak is potentially much larger than currently detected.
Furthermore, the outbreak has spread to Bunia, a densely populated provincial capital. Urban transmission is far more dangerous than rural spread because of the higher population density and mobility.
High-Risk Factors: The Perfect Storm
Beyond the virus itself, several environmental factors make this outbreak particularly challenging to contain:
1. Healthcare Worker Deaths
Four healthcare workers are among the deceased. This is a red flag indicating significant gaps in infection prevention and control (IPC) within hospitals and clinics, which can turn medical facilities into amplification points for the virus.
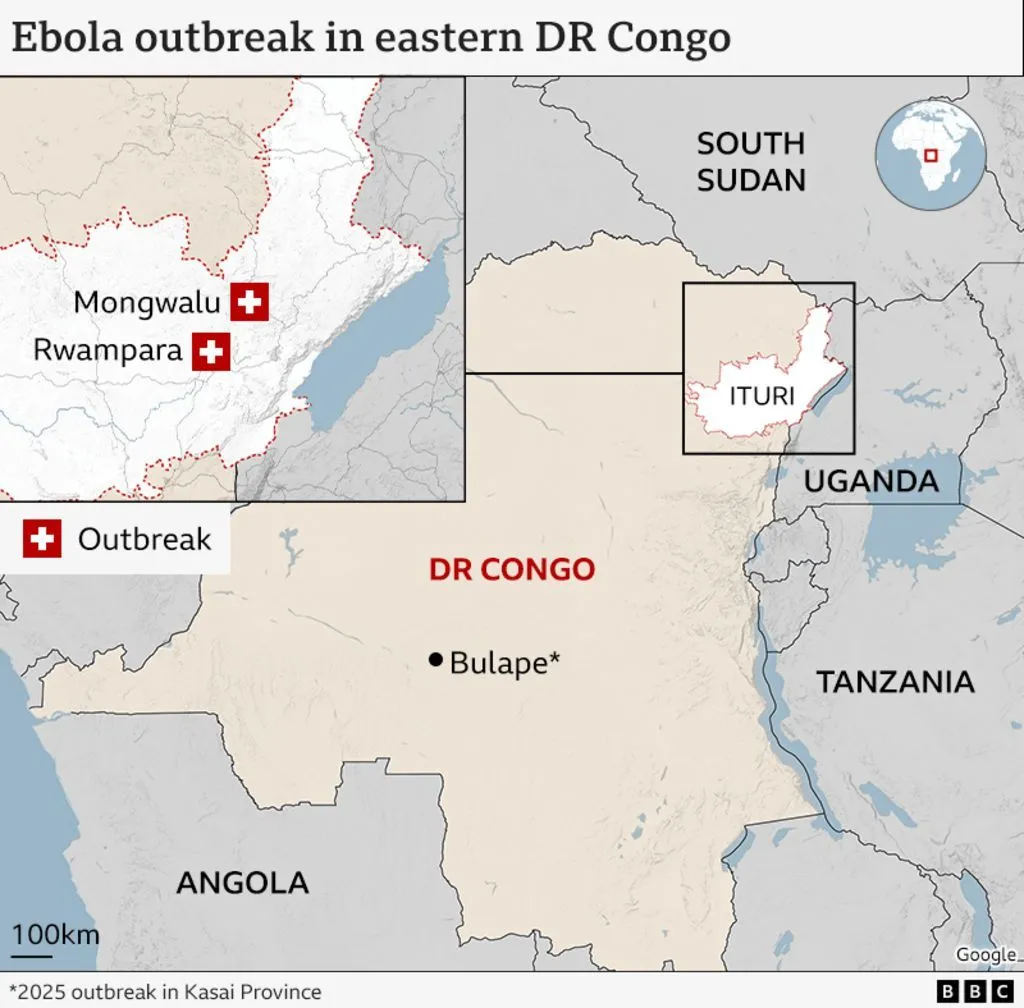
2. Insecurity and Population Movement
The outbreak is occurring in Ituri Province, an area plagued by ongoing insecurity and humanitarian challenges. The affected zone of Mongwalu is a high-traffic mining area with intense population mobility. People are constantly moving for work, trade, and to seek medical care, making contact tracing extremely difficult.
3. The Risk of Regional Spread
The DRC shares borders with Uganda, South Sudan, Rwanda, and Burundi. Given the trade and travel links, neighboring countries are considered at high risk. Uganda has already confirmed two imported cases in the capital city of Kampala.
In Context: This is the 17th Ebola outbreak in the DRC since the virus was first identified there in 1976. The DRC actually has a “strong track record” in Ebola response and has significant expertise in containing these outbreaks.
How Worried Should You Be? (By Region)
The level of worry depends entirely on where you live or plan to travel.
For people in the EU/EEA, the US, or Asia:
Risk Level: VERY LOW
The European Centre for Disease Prevention and Control (ECDC) states that the “likelihood of infection for people living in the EU/EEA is considered very low”. The WHO has assessed the global risk as “low” . Unless you have direct contact with an infected person’s bodily fluids while traveling in the affected zone, your daily life is unaffected.
For travelers planning to visit DRC or Uganda:
Risk Level: MODERATE (Specific to Ituri)
Taiwan’s CDC has raised the travel advisory for DRC and Uganda to Level 2: “Alert” . You should avoid non-essential travel to Ituri Province. If you must go, avoid contact with sick people, avoid bushmeat, and practice rigorous hand hygiene.
For people living in Ituri Province, DRC, or border regions of Uganda:
Risk Level: HIGH
This is the epicenter. The Africa CDC rates the risk as “very high” for DRC and high for Eastern Africa. Residents should strictly follow guidance from health authorities, report symptoms immediately, and avoid physical contact with suspected cases or deceased bodies.
The Response: What is Being Done?
Despite the challenges, a massive response is underway.
- Emergency Declaration: The PHEIC declaration allows for more international funding and coordination.
- Rapid Response Teams: WHO, Africa CDC, and MSF have deployed teams to the ground to support surveillance, contact tracing, and case management.
- Research Acceleration: Africa CDC has activated a workstream to assess potential medical countermeasures. While no vaccine exists yet, research teams are beginning to plan studies. The goal is to not just contain this outbreak, but to finally develop tools against this neglected strain.
Practical Advice for Travelers and Residents
- Avoid non-essential travel to Ituri Province in DRC.
- Practice strict hand hygiene (use soap or alcohol-based sanitizers).
- Avoid contact with anyone showing symptoms (fever, vomiting, diarrhea, unexplained bleeding).
- Avoid bushmeat and contact with bats or non-human primates.
- If you develop symptoms (especially fever) within 21 days of returning from the region, isolate immediately and call a doctor. Do not go to the waiting room unannounced (call ahead to warn them of your travel history).
The Bottom Line
The 2026 Bundibugyo virus outbreak is very worrying for the people of eastern DRC and their neighbors. The lack of a vaccine, the urban spread, and the complex security situation create a genuine risk of a large regional epidemic.
However, for the rest of the world, the situation is not a cause for panic. Global health systems are vigilant, screening is in place, and the risk of widespread international transmission remains very low. The focus right now is on supporting the DRC and Uganda to do what they have done 16 times before: stop the virus through the hard work of public health, one contact at a time.
Ebola Vaccine Effectiveness & Strain Coverage
The effectiveness of Ebola vaccines depends heavily on which viral strain you’re talking about. Currently, licensed vaccines only exist for the Zaire ebolavirus (the strain responsible for the 2014-2016 West Africa epidemic). For other strains, like the Sudan virus or the Bundibugyo virus causing the 2026 outbreak, no approved vaccines are available yet.
How Effective Are the Licensed Zaire Ebola Vaccines?
There are two main vaccine regimens approved for Zaire ebolavirus:
1. rVSV-ZEBOV (Single-dose)
- Brand name: Ervebo®
- Approved in: USA, EU, Canada, and several African countries
- Dosing: One intramuscular injection
2. Ad26.ZEBOV + MVA-BN-Filo (Two-dose)
- Brand names: Zabdeno® (Ad26.ZEBOV) and Mvabea® (MVA-BN-Filo)
- Approved in: EU, used in DRC outbreaks
- Dosing: Two injections given 56 days apart
Key effectiveness data:
The immune response is highly specific to Zaire ebolavirus—studies show minimal cross-reactivity to other Ebola species, meaning these vaccines will not protect against Sudan or Bundibugyo strains.
What About Other Ebola Strains?
Here is the current status of vaccines for other Ebola virus species:
Why Is the Bundibugyo Outbreak a Concern?
The current outbreak in Ituri Province, DRC (declared May 15, 2026) involves the Bundibugyo strain. As DRC Health Minister Samuel-Roger Kamba stated, this strain has “no vaccine and no specific treatment” and carries a “very high lethality rate which can reach 50%”.
Without a vaccine, outbreak control relies entirely on traditional public health measures:
- Isolation of confirmed cases
- Contact tracing
- Safe burial practices
- Infection prevention and control in healthcare settings
This is why the WHO declared the outbreak a Public Health Emergency of International Concern (PHEIC).
The Future: Multivalent Vaccines
Research is actively pursuing vaccines that can protect against multiple Ebola strains simultaneously. The Janssen vaccine (Ad26.ZEBOV + MVA-BN-Filo) includes components targeting Sudan and Marburg viruses, but studies show the antibody response remains largely Zaire-specific. Scientists conclude that different multivalent vaccine candidates are required to provide broad protection across filoviruses.
The Uganda Sudan virus vaccine trial launched in 2025 is a critical step toward filling this gap.
Summary Table: Vaccine Coverage by Strain
| Category | Do This | Avoid This |
|---|---|---|
| Hygiene | Wash hands frequently with soap or sanitizer. | Touching eyes, nose, or mouth with unwashed hands. |
| Food | Eat thoroughly cooked food. | Bushmeat, raw meat, or contact with bats/monkeys. |
| Social | Stay 3 feet away from sick individuals. | Physical contact with corpses or burial rituals. |
| Travel | Get travel health insurance with evacuation. | Non-essential travel to Ituri Province (Level 4). |
| Medical | Call the hospital before arriving if sick. | Visiting local hospitals or traditional healers for minor issues. |
| Ebola Strain | Licensed Vaccine? | Protection Status |
|---|---|---|
| Zaire | ✅ Yes | Protected |
| Sudan | ❌ No | In clinical trial (2025) |
| Bundibugyo | ❌ No | No vaccine available |
| Tai Forest | ❌ No | Investigational only |
Bottom Line
The existing Ebola vaccines are highly effective against the Zaire strain, with strong antibody responses in over 99% of recipients and protection lasting at least a year. However, they do not protect against other Ebola species. For the Bundibugyo strain causing the current DRC outbreak, there is no vaccine—making this outbreak particularly dangerous and difficult to contain.
what are the precautions for this epidemic
Read 10 web pages
Given that the current outbreak involves the Bundibugyo strain, for which there is no licensed vaccine or specific treatment, precautions are currently the most critical line of defense . Here is a comprehensive guide to protecting yourself and others, whether you are in the affected region or traveling internationally.
1. Understand How It Spreads (And How It Does Not)
The virus is not airborne like the flu or COVID-19 . Infection requires direct contact with:
- Blood or bodily fluids (urine, saliva, sweat, vomit, diarrhea, breast milk, semen) of an infected person or corpse.
- Contaminated objects (needles, bedding, clothing).
- Infected wildlife (fruit bats, primates, forest antelopes) or their raw meat .
2. Precaution Measures for Travelers & Expats
If you are in or traveling to the DRC or Uganda, follow these health and safety protocols:
Avoid Direct Contact
- Do not touch a person showing symptoms (fever, weakness, vomiting, diarrhea, unexplained bleeding).
- Do not touch a corpse or participate in burial rituals that involve physical contact with the deceased.
- Do not touch bedding, clothing, or medical equipment that may have been contaminated.
Avoid High-Risk Wildlife & Food
- Stay away from bats, monkeys, chimpanzees, and gorillas.
- Avoid caves or mines where bats might roost.
- Do not eat bushmeat (wild animal meat).
- Wash hands frequently with soap and water or use an alcohol-based sanitizer.
Healthcare & Travel Logistics
- Avoid non-essential visits to local hospitals or traditional healers in the affected zones to prevent exposure to unsterilized equipment .
- Check your insurance: Ensure you have medical evacuation coverage before traveling, as local facilities may be overwhelmed .
- Follow travel advisories: The U.S. CDC has issued a Level 2 Alert (Practice Enhanced Precautions) for the DRC and Uganda, with a Level 4 “Do Not Travel” advisory specifically for Ituri Province .
3. Symptom Monitoring & What To Do If You Feel Sick
Ebola has a 21-day incubation period (you will not show symptoms immediately) .
Immediate Protocol (If you develop fever, headache, muscle pain, vomiting, or bleeding):
- Isolate yourself immediately from others.
- Do not travel on public transport or commercial planes .
- Call before you go: If you seek medical care, call the clinic or hospital first. This allows them to prepare isolation protocols so they don’t expose other patients or staff .
- Mention your travel history to doctors immediately.
- Continue malaria prophylaxis: Malaria symptoms mimic Ebola (fever/body aches). Preventing malaria reduces the chance of a false alarm health scare .
4. Border & Household Hygiene
For those living in neighboring countries (like Burundi, Rwanda, or South Sudan), the risk is higher due to cross-border mobility . Authorities are implementing:
- Temperature screening at airports and major land crossings .
- Public awareness campaigns on the importance of safe burials and handwashing.
- One Health surveillance to monitor animal health as a warning system .
For Households:
- If caring for a sick person, wear gloves and masks.
- Disinfect surfaces with bleach solutions (the virus is easily killed by disinfectants).
- Wash soiled clothing/linens with hot water and detergent without directly touching them.
5. Post-Travel Protocol (For Global Travelers)
If you return home from DRC or Uganda:
- Monitor your health for 21 days.
- If you develop a fever, immediately call your local health department or emergency number (e.g., 1922 in Taiwan) before going to a hospital .
- Tell the operator you have been in an Ebola outbreak zone.
Summary of Key Action Points
Because there is no vaccine for the Bundibugyo strain, early supportive care is the only lifesaving treatment . If you feel symptoms, do not wait; seek professional help immediately following the “call first” rule.
⚠️ Educational only: Not medical advice. If exposed or symptomatic (fever, vomiting, bleeding), call your local health authority immediately — do not go to a clinic without calling first. Always follow official WHO/CDC/Ministry of Health guidance.

