For decades, diagnosing a neurodegenerative disease was a grim exercise in watching and waiting. A patient would arrive with memory lapses, a tremor, or a change in personality. The neurologist would perform cognitive tests, review the patient’s history, and say, “It looks like Alzheimer’s” or “This is likely Parkinson’s.” But the truth was uncomfortable: without an autopsy, no one could be 100% certain. Fluid Biomarkers for Neurodegenerative Diseases: A Complete Diagnostic Guide can change the way neurodegenerative diseases are diagnosed.
That era is ending. Thanks to rapid advances in molecular medicine, fluid biomarkers for the diagnosis of neurodegenerative diseases have transformed the field from a probabilistic art into a precision science. Today, a simple spinal tap or even a blood draw can reveal the invisible pathology brewing inside a living brain—years before the first symptom ever appears.
Part 1: What Are Fluid Biomarkers?
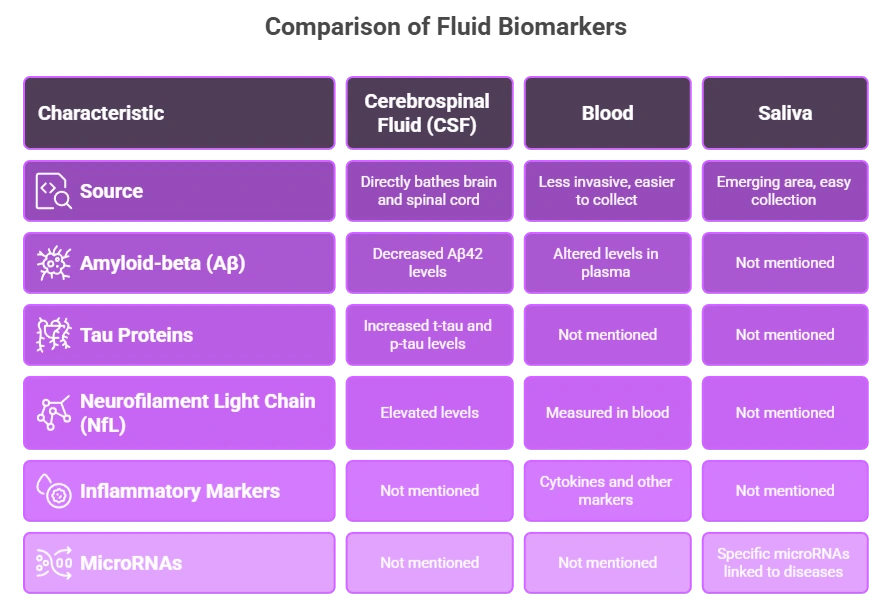
A biomarker (biological marker) is a measurable indicator of a normal or abnormal biological process. In the context of neurodegeneration, fluid biomarkers are molecules found in bodily fluids—most commonly cerebrospinal fluid (CSF) and blood—that reflect what is happening in the brain.
Think of them as the brain’s “molecular smoke alarm.” When neurons are injured, misfolded proteins accumulate, or synapses degenerate, these events leave chemical traces that diffuse into the CSF and eventually into the bloodstream.
The most valuable fluid biomarkers for the diagnosis of neurodegenerative diseases fall into three categories:
| Category | What They Measure | Examples |
|---|---|---|
| Amyloid/tau markers | Alzheimer’s-specific pathology | Aβ42, Aβ40, p-tau181, t-tau |
| Neuroaxonal injury markers | General neuronal damage | Neurofilament light chain (NfL) |
| Neuroinflammation markers | Immune activity in the brain | GFAP, YKL-40, sTREM2 |
Part 2: Cerebrospinal Fluid – The Gold Standard
Cerebrospinal fluid (CSF) bathes the brain and spinal cord. Because it is in direct contact with brain tissue, CSF provides the most accurate reflection of central nervous system pathology. A lumbar puncture (spinal tap) collects approximately 10–15 mL of fluid, which is then analyzed using highly sensitive immunoassays or mass spectrometry.
Alzheimer’s Disease: The Prototypical Success Story
No other neurodegenerative disease has benefited more from fluid biomarkers than Alzheimer’s. The core pathology involves:
- Amyloid-beta plaques (extracellular protein clumps)
- Tau neurofibrillary tangles (inside neurons)
The classic CSF biomarker profile for Alzheimer’s disease includes:
- Low Aβ42 (because it is trapped in plaques, not free in fluid)
- High p-tau181 (hyperphosphorylated tau released from tangles)
- High t-tau (total tau, reflecting general neuronal death)
This profile now has over 90% sensitivity and specificity for identifying Alzheimer’s pathology, even in patients with mild cognitive impairment. In fact, the 2018 National Institute on Aging–Alzheimer’s Association (NIA-AA) research framework redefined Alzheimer’s as a biological construct—meaning you can diagnose it with biomarkers alone, without waiting for clinical dementia.
Beyond Alzheimer’s: Other Diseases
Fluid biomarkers for the diagnosis of neurodegenerative diseases are not limited to Alzheimer’s:
- Parkinson’s disease and dementia with Lewy bodies: Low CSF α-synuclein levels (often combined with normal Aβ42 and p-tau) help differentiate these from Alzheimer’s.
- Creutzfeldt-Jakob disease (CJD): Extremely high CSF tau (>1200 pg/mL) and the presence of 14-3-3 protein are diagnostic.
- Multiple system atrophy (MSA): Low CSF α-synuclein but with distinct co-pathologies.
- Frontotemporal dementia (FTD): Normal or mildly abnormal Alzheimer’s markers, but research biomarkers like TDP-43 and progranulin are emerging.
Part 3: The Game-Changer – Blood-Based Biomarkers
For years, the need for a lumbar puncture limited the widespread use of fluid biomarkers. Many patients feared the procedure. Many primary care clinics could not perform it. That barrier is now crumbling.
Recent technological advances—specifically, ultra-sensitive immunoassays (Simoa, Elecsys) and mass spectrometry—have made it possible to detect brain-derived proteins in blood, even at extremely low concentrations.
The Star Performer: Neurofilament Light Chain (NfL)
Neurofilament light chain (NfL) is a structural protein inside large-caliber axons. When any axon is damaged—whether by Alzheimer’s, multiple sclerosis, stroke, or traumatic brain injury—NfL leaks out and can be measured in both CSF and blood.
Elevated blood NfL is a non-specific but highly sensitive marker of neuroaxonal injury. It cannot tell you which disease a patient has, but it can tell you:
- That something is damaging the brain
- How rapidly the damage is progressing
- Whether a treatment is slowing that damage
In clinical practice, a patient with cognitive complaints and a normal blood NfL is very unlikely to have a rapidly progressive neurodegenerative disease. Conversely, an elevated NfL demands further investigation.
Alzheimer’s-Specific Blood Markers
Remarkably, we can now measure the same Alzheimer’s proteins in blood that we once needed CSF for:
- Plasma p-tau181, p-tau217, and p-tau231: These phosphorylated tau species are highly specific for Alzheimer’s pathology. Plasma p-tau217, in particular, distinguishes Alzheimer’s from other dementias with accuracy approaching 95%.
- Plasma Aβ42/Aβ40 ratio: A low ratio indicates brain amyloid deposition, but blood measurements are more challenging and less accurate than CSF.
- Plasma GFAP (glial fibrillary acidic protein): An emerging marker of astrocytic activation (neuroinflammation), which rises early in Alzheimer’s.
Part 4: How Fluid Biomarkers Change Clinical Practice
The integration of fluid biomarkers for the diagnosis of neurodegenerative diseases has created four paradigm shifts:
1. Early and Accurate Diagnosis
Before biomarkers, up to 30% of clinical diagnoses of Alzheimer’s were wrong—patients instead had frontotemporal dementia, Lewy body dementia, or even depression. Fluid biomarkers cut that error rate dramatically. A patient with atypical symptoms (e.g., language problems rather than memory loss) can now receive a definitive biological diagnosis.
2. Preclinical Detection
We now know that Alzheimer’s pathology begins 15 to 20 years before dementia. Fluid biomarkers can detect amyloid accumulation in cognitively normal individuals. This is not a diagnosis of disease—many people with amyloid never progress—but it enables research into prevention trials and risk stratification.
3. Differential Diagnosis of Parkinsonism
Distinguishing Parkinson’s disease from atypical parkinsonian syndromes (multiple system atrophy, progressive supranuclear palsy, corticobasal degeneration) is notoriously difficult. CSF markers—especially α-synuclein seeding amplification assays (real-time quaking-induced conversion, or RT-QuIC)—now achieve near-perfect specificity. A positive α-synuclein seed amplification test confirms Parkinson’s or Lewy body dementia.
4. Monitoring Treatment Response
As disease-modifying therapies emerge—such as anti-amyloid antibodies (lecanemab, donanemab)—fluid biomarkers serve as pharmacodynamic measures. A successful drug should lower p-tau and NfL in the blood or CSF over time. If biomarkers do not change, the drug is likely failing, even if the patient feels stable in the short term.
Part 5: Limitations and Challenges
No diagnostic tool is perfect. Fluid biomarkers for the diagnosis of neurodegenerative diseases face several hurdles:
- Invasiveness: Lumbar puncture remains a barrier for many patients, though serious complications are rare (post-dural headache in 1–2%).
- Cost and accessibility: CSF analysis is expensive ($500–1500 USD) and not universally available. Blood tests are cheaper but still not covered by all insurance systems.
- Reference ranges: Values vary by age, assay, and laboratory. A “normal” p-tau level at age 70 may be abnormal at age 50.
- Comorbidities: Kidney disease can affect blood NfL levels. Chronic inflammation can alter GFAP. Interpretation requires clinical context.
- Not all diseases have biomarkers: For Huntington’s disease, genetic testing remains the gold standard. For many rare dementias, fluid biomarkers are still research tools.
Part 6: The Future – Next-Generation Fluid Biomarkers
The field is evolving rapidly. Several exciting developments are on the horizon:
- Blood NfL as a screening tool: Some experts envision measuring NfL in routine annual blood work for adults over 60. An unexplained rise would trigger a cognitive evaluation and more specific biomarkers.
- Phosphorylated tau isoforms: p-tau217 appears to track amyloid pathology more closely than tau tangles; p-tau231 rises even earlier. Combinations of isoforms may map disease stage.
- Synaptic biomarkers: Neurogranin, SNAP-25, and GAP-43 reflect synapse loss—potentially a more direct correlate of cognitive decline than amyloid or tau.
- Extracellular vesicles (EVs): Small particles shed from brain cells can be isolated from blood. Analyzing their internal contents (proteins, RNA, lipids) offers a window into cell-type-specific pathology.
- Liquid biopsy for prion diseases: RT-QuIC assays can now detect misfolded α-synuclein and tau in CSF and even blood, opening the door to early diagnosis of Parkinson’s, Lewy body dementia, and progressive supranuclear palsy.
Conclusion: From Mystery to Measurement
The arrival of fluid biomarkers for the diagnosis of neurodegenerative diseases has changed the conversation between neurologist and patient. No longer must a family hear, “We think it’s Alzheimer’s, but we can’t be sure.” Today, a lumbar puncture or a blood draw can provide a molecular diagnosis, a prognosis, and a pathway to clinical trials.
Are there limitations? Absolutely. Not every clinic has access. Not every patient wants a spinal tap. And no biomarker can yet reverse a single symptom. But for the first time in history, we can see the enemy. We can measure it, track it, and—in the case of anti-amyloid therapies—fight it with precision.
The brain is no longer a black box. Its secrets are leaking into the fluid around it, and we are finally learning to read the signs.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Fluid biomarker testing, including CSF analysis and blood-based assays, should be ordered and interpreted by a qualified neurologist or physician. Do not use this information to self-diagnose or alter any treatment plan. Always consult a healthcare professional for medical concerns.