Cancer risk arises from a complex interplay between genes, environment, and lifestyle. Among these, genetic predisposition stands out as a major non-modifiable risk factor—you cannot change the DNA you inherit, but you can identify, quantify, and act on that risk. This reality has made hereditary cancer risk a central pillar of contemporary prevention science.
🧬 What Is Genetic Predisposition?
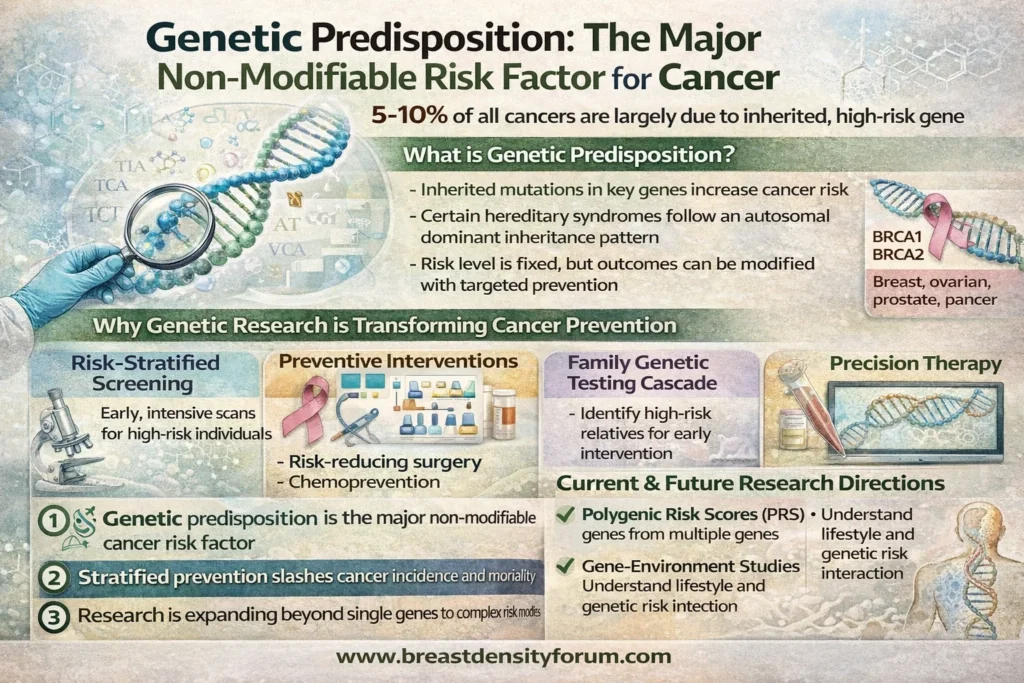
Genetic predisposition refers to inherited variants (mutations) in specific genes that increase the likelihood of developing cancer. These variants are typically passed down in families and may follow autosomal dominant inheritance (a single altered copy is sufficient to elevate risk).
Key high-penetrance examples include:
- BRCA1 and BRCA2 → breast, ovarian, pancreatic, prostate cancers
- TP53 → Li-Fraumeni syndrome (multiple early-onset cancers)
- MLH1 and MSH2 → Lynch syndrome (colorectal, endometrial, others)
These genes typically function as tumor suppressors or DNA repair proteins. When impaired, cells accumulate mutations more rapidly—accelerating carcinogenesis.
📊 How Much Cancer Is Genetic?
- Roughly 5–10% of all cancers are strongly hereditary (high-penetrance mutations)
- A larger fraction (20–30%) shows familial clustering, reflecting moderate-risk genes + shared environment
- The remainder are largely sporadic, driven by acquired mutations over time
Despite being a minority numerically, hereditary cancers are disproportionately important because they are predictable and actionable.
🔬 Why Genetic Risk Is Central to Prevention Research
1) Risk Stratification & Precision Screening
Genetic data enables risk-adapted screening:
- Earlier and more frequent imaging for high-risk individuals
- Tailored modalities (e.g., MRI vs mammography in high-risk breast cohorts)
2) Preventive Interventions
Evidence-based options include:
- Risk-reducing surgeries (e.g., prophylactic mastectomy/oophorectomy in BRCA carriers)
- Chemoprevention (e.g., selective estrogen receptor modulators in high-risk breast cancer)
- Intensive surveillance programs
3) Family Cascade Testing
Identifying one carrier enables testing of relatives, amplifying prevention impact across families.
4) Therapeutic Implications
Genetics informs treatment (e.g., PARP inhibitors in BRCA-mutated cancers), linking prevention and precision oncology.
🧪 Expanding Frontier: From Single Genes to Polygenic Risk
While classic syndromes involve single high-impact genes, current research is rapidly advancing:
Polygenic Risk Scores (PRS)
- Aggregate hundreds to thousands of common variants
- Provide graduated risk estimates in the general population
- Enable population-level stratified screening programs
Multi-Omics Integration
- Combining genomics with epigenomics, transcriptomics, and proteomics
- Aims to detect pre-clinical disease signals before symptoms arise
🧠 Gene–Environment Interaction: Risk Is Not Destiny
Even with high-risk mutations, penetrance is variable. Environmental and lifestyle factors modulate risk:
- Tobacco exposure, diet, obesity, infections (e.g., HPV), and reproductive factors
- Hormonal milieu and inflammation
- Access to screening and healthcare
This interplay underscores a crucial principle:
👉 Genetic risk is fixed—but outcomes are modifiable.
🧬 Testing & Counseling: The Clinical Workflow
Who Should Be Tested?
- Early-onset cancers
- Multiple related cancers in a family
- Known familial mutation
- Specific tumor types (e.g., triple-negative breast cancer)
How It’s Done
- Blood/saliva-based germline genetic testing
- Interpreted alongside genetic counseling to manage uncertainty (e.g., variants of uncertain significance)
⚖️ Ethical, Social, and Practical Considerations
- Psychological impact (anxiety, decision burden)
- Privacy and discrimination concerns
- Cost and access disparities
- Need for culturally sensitive counseling and equitable screening programs
🚀 The Future of Cancer Prevention
Research priorities are converging on:
- Population-scale genomic screening integrated into primary care
- AI-driven risk models combining genetics, imaging, and lifestyle data
- Liquid biopsies for ultra-early detection
- Personalized prevention pathways rather than one-size-fits-all screening
Global guidance from bodies like the World Health Organization and oncology societies increasingly supports risk-stratified approaches as evidence matures.
🧾 Key Takeaways
- Genetic predisposition is the leading non-modifiable cancer risk factor
- It is highly actionable, making it a cornerstone of prevention research
- Advances like PRS and multi-omics are expanding risk prediction beyond rare syndromes
- Early identification + tailored intervention can substantially reduce cancer incidence and mortality
🩺 Bottom Line
You cannot change your genes—but modern medicine can read them, interpret them, and act on them. As a result, genetic predisposition has shifted from a static risk factor to a dynamic opportunity for prevention, reshaping how we approach cancer risk in 2026 and beyond.