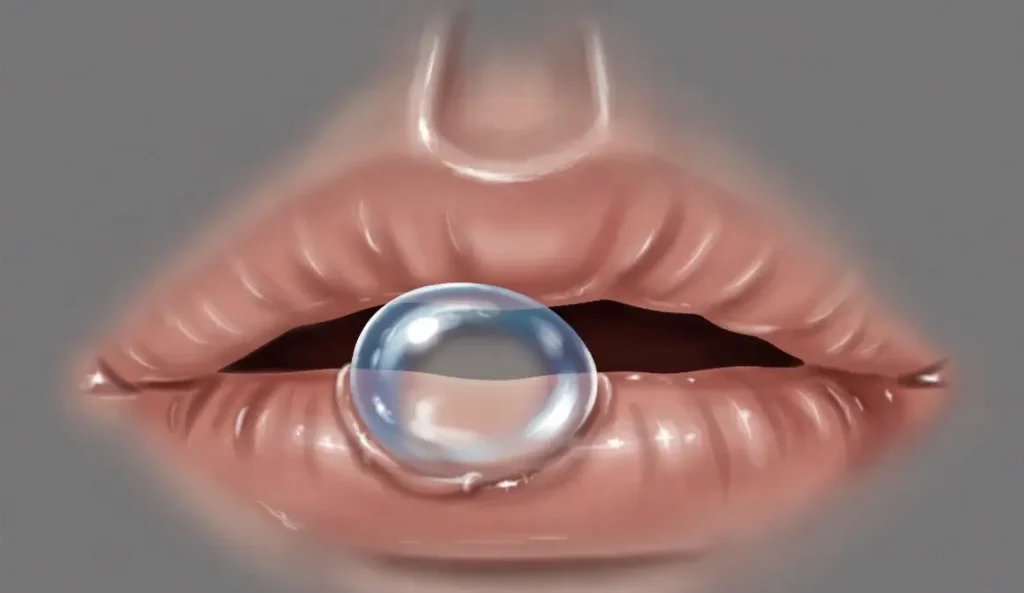
You are eating dinner, and suddenly you feel a small, soft bump on the inside of your lip. You look in the mirror and see a tiny, bluish blister. What is it? Chances are, you have an oral mucocele.
These common, benign cysts affect approximately 2.4 out of every 1,000 people . While they are usually harmless, many people panic, wondering if their oral mucocele cancer risk is real.
This comprehensive guide covers everything you need to know about oral mucoceles—from oral mucocele symptoms and causes to the full range of oral mucocele treatments, including oral mucocele surgery and supportive care. We will also address the critical question: Can an early stage oral mucocele cancer be mistaken for a simple cyst?
Part 1: What Is an Oral Mucocele?
An oral mucocele is a painless, fluid-filled swelling (cyst) on the inner surface of the mouth. The term comes from Latin—”mucus” and “coele,” meaning cavity . These cysts occur when a minor salivary gland becomes damaged or blocked, causing saliva to pool in the surrounding tissue .
Other names for oral mucoceles include:
How Common Are Oral Mucoceles?
Oral mucoceles are the most common lesion of the minor salivary glands . They account for the 17th most common type of lesion in the oral cavity . The prevalence in the general population ranges from 0.4% to 0.9%, though US statistics show approximately 2.5 lesions per 1,000 people .
Who Gets Oral Mucoceles?
While oral mucoceles can affect anyone, they are most common in younger people. Individuals between the ages of 3 and 20 make up about 70% of cases, with the peak occurrence between 10 and 20 years old . There is no gender predilection—males and females are equally affected .
The Two Types of Oral Mucoceles
There are two primary types of oral mucoceles :
| Type | Frequency | Cause | Common Location |
|---|---|---|---|
| Extravasation Mucocele | ~84% of cases | Ruptured salivary duct leaks saliva into surrounding tissue | Lower lip |
| Retention Mucocele | ~16% of cases | Blocked salivary duct (stone or thickened mucus) | Upper lip, palate, floor of mouth |
The extravasation type is far more common, especially in children and young adults .
Part 2: Oral Mucocele Symptoms
Recognizing oral mucocele symptoms is the first step toward proper treatment. Most mucoceles are easy to identify by their appearance.
Classic Oral Mucocele Symptoms
Deeper or Chronic Mucoceles
Mucoceles located deeper within the tissue may present differently:
- Rounded shape with a whitish color
- Tenderness to touch
- Firmer consistency (due to fibrosis from repeated rupture)
Ranula: A Special Type of Mucocele
When an oral mucocele occurs on the floor of the mouth, it is called a ranula (from the Latin for “little frog,” due to its resemblance to a frog’s air sac) . Ranula symptoms include:
- Bluish, dome-shaped swelling under the tongue
- Usually painless but can interfere with chewing, swallowing, or talking if large
- In rare cases, can grow into the neck and cause breathing difficulty (a medical emergency)
Do Oral Mucoceles Rupture on Their Own?
Yes. Many oral mucoceles will spontaneously rupture, releasing their clear, viscous fluid. The swelling then disappears. However, because the underlying damaged gland remains, the cyst often recurs—sometimes repeatedly .
Part 3: What Causes Oral Mucoceles?
Understanding the cause helps with prevention and treatment planning.
Trauma Is the #1 Cause
The most common cause of an oral mucocele is physical trauma to the minor salivary glands . Specific causes include:
- Lip biting (accidental or habitual) – the most frequent cause
- Cheek biting or sucking – a common habit, especially during sleep
- Lip sucking – a parafunctional habit
- Trauma from dental procedures or intubation
- Long-term irritation from smoking or tobacco products
Other Causes
- Blocked salivary ducts due to thickened mucus or salivary stones (sialoliths)
- Irritation from dental products – some tartar-control toothpastes or antiseptic mouthwashes may contribute to duct narrowing
- Lip or tongue piercings that rub against oral tissues
The “Why Lower Lip?” Question
The lower lip is the most common location for oral mucoceles because it is the most frequently traumatized area during chewing and biting . The proximity of minor salivary glands to the surface makes them vulnerable to injury.
Part 4: Oral Mucocele Cancer Risk – What You Need to Know
This is the question that causes the most anxiety: Is oral mucocele cancer possible?
The Short Answer
Oral mucocele cancer is extremely rare. Oral mucoceles are benign (non-cancerous) lesions. They are not a form of cancer, and they do not typically transform into cancer .
However, there is a critical nuance: Other, more serious conditions can look like mucoceles.
When to Suspect Something More Serious
According to medical literature, the differential diagnosis for an oral mucocele includes several other conditions, some of which are malignant :
Early Stage Oral Mucocele Cancer – Does It Exist?
Early stage oral mucocele cancer is not a standard diagnosis because mucoceles themselves are not cancer. However, early stage oral cancer (specifically salivary gland cancers like mucoepidermoid carcinoma) can sometimes mimic a mucocele in appearance.
Red flags that warrant a biopsy include :
- Cyst larger than 2 centimeters (0.8 inches)
- Firm or hard consistency (mucoceles are soft)
- Lesion that persists for more than 2 months without changing
- History of the lesion growing steadily (rather than rupturing and recurring)
- Pain or tenderness (though some cancers are also painless early on)
- Location on the palate or upper lip (less common for benign mucoceles)
The Biopsy Protocol
If your healthcare provider has any suspicion, they will order a biopsy—removing a small tissue sample for examination under a microscope. This is the only definitive way to rule out malignancy .
The takeaway: Most oral bumps are benign mucoceles. But any oral lesion that does not heal or resolve within 2-4 weeks should be evaluated by a dentist or doctor.
Part 5: Oral Mucocele Supportive Therapy and Home Care
For most small, painless mucoceles, no active treatment is needed. However, oral mucocele supportive therapy can help speed healing and prevent complications.
What NOT to Do
Never try to pop, cut, or drain an oral mucocele at home. Attempting how to get rid of oral mucocele through DIY methods can lead to:
- Secondary infection
- Scarring and fibrosis (making future treatment harder)
- Damage to surrounding salivary glands
- Recurrence (often worse than the original)
Safe Supportive Therapies
If you want to support natural healing, these methods are generally considered safe:
How Long Does Healing Take?
If left alone, most oral mucoceles will rupture and heal on their own within 3 to 6 weeks . If the cyst persists beyond 2 months without rupturing, or if it continues to recur frequently, medical treatment should be considered.
The Role of Observation
For many patients, the best oral mucocele supportive therapy is simply “watchful waiting.” The cyst may disappear and never return. Even if it recurs, it often does so intermittently and may eventually resolve as the damaged gland heals .
Part 6: Oral Mucocele Treatment – Professional Options
When a mucocele is large, painful, persistent, or recurrent, professional oral mucocele treatment is indicated. Multiple options exist, ranging from minimally invasive to surgical.
Overview of Oral Mucocele Treatments
| Treatment | Method | Best For | Recurrence Risk |
|---|---|---|---|
| Observation | Do nothing; wait for spontaneous rupture | Small, painless, first-time lesions | High (if gland remains damaged) |
| Cryotherapy | Freeze cyst with liquid nitrogen | Small, superficial mucoceles | Low to moderate |
| Laser treatment | Ablate cyst with CO2 or diode laser | Small to moderate lesions | Low to moderate |
| Surgical excision | Cut out cyst AND associated minor salivary glands | Recurrent or large mucoceles | Very low (5-10%) |
| Marsupialization | Create a permanent opening to allow drainage | Ranulas (floor of mouth) | Moderate |
| Intralesional injection | Inject sclerosing agent (e.g., 2% iodine) | Patients who cannot undergo surgery | Variable |
Oral Mucocele Surgery – What to Expect
Oral mucocele surgery is the most definitive treatment, especially for recurrent lesions. The procedure involves:
- Anesthesia: Local anesthetic is injected to numb the area
- Excision: The surgeon cuts out the entire cyst AND the associated minor salivary glands (to prevent recurrence)
- Closure: The wound is usually closed with dissolvable sutures
- Recovery: Soft diet for several days; healing takes 1-2 weeks
Success rate: Surgical excision has the lowest recurrence rate, though studies report recurrence in up to 25% of cases if gland remnants remain .
Less Invasive Options
For patients who want to avoid oral mucocele surgery, these alternatives may be appropriate:
Cryotherapy:
- Liquid nitrogen freezes and destroys the cyst
- Quick procedure (minutes)
- Minimal discomfort
- May require multiple sessions
Laser Treatment:
- CO2 or diode laser vaporizes the cyst
- Precise, minimal bleeding
- Faster healing than surgery
- Slightly higher recurrence rate than excision
Oral Mucocele Treatment for Ranulas
Ranulas (mucoceles on the floor of the mouth) often require more aggressive treatment because of their location and potential to interfere with breathing. Treatment options include:
- Marsupialization (creating a permanent drainage opening)
- Complete excision of the cyst AND the sublingual gland (highest success rate)
Part 7: How to Get Rid of Oral Mucocele – A Step-by-Step Guide
When patients search for how to get rid of oral mucocele, they want a clear action plan. Here is a medical-grade approach:
Step 1: Confirm It Is a Mucocele
Before any treatment, get a professional diagnosis. A dentist or doctor can usually identify an oral mucocele by sight and history alone. If there is any doubt, they may order imaging (ultrasound) or a biopsy.
Step 2: Try Watchful Waiting (2 months)
For a first-time, small, painless mucocele:
- Leave it alone
- Avoid lip biting and cheek sucking
- Use warm salt water rinses
- Monitor for spontaneous rupture
Expected outcome: 70-80% will resolve on their own within 3-6 weeks .
Step 3: Seek Treatment If Persistent
If the cyst persists beyond 2 months, recurs frequently, or causes discomfort:
- Schedule an appointment with an oral surgeon or dentist
- Discuss which treatment option is best for your situation
Step 4: Choose a Treatment
| If you want… | Choose… |
|---|---|
| The lowest recurrence risk | Surgical excision |
| Minimal invasiveness | Cryotherapy or laser |
| To avoid surgery entirely | Observation or intralesional injection |
Step 5: Prevent Recurrence
After successful treatment, prevent future oral mucoceles by:
- Stopping lip/cheek biting habits (behavioral modification)
- Quitting smoking or tobacco use
- Maintaining excellent oral hygiene (to prevent duct blockage)
- Using a soft toothbrush to avoid trauma
Part 8: Prevention – Stopping Oral Mucoceles Before They Start
The best treatment is prevention. Since trauma is the #1 cause, reducing oral injury is key.
Actionable Prevention Strategies
The Lip Biting Connection
Lip biting is responsible for the vast majority of oral mucoceles, especially on the lower lip . If you notice that your cyst appears after a meal where you bit your lip—or if you have a chronic lip-biting habit—breaking that habit is your most powerful prevention tool.
Part 9: When to See a Doctor
Most oral mucoceles are harmless and self-limiting. However, certain signs warrant professional evaluation.
See a Dentist or Doctor If:
- The cyst persists for more than 2 months without changing
- The cyst is larger than 2 centimeters (about 0.8 inches)
- You have difficulty talking, chewing, or swallowing
- You experience pain (mucoceles are usually painless)
- The cyst has a firm or hard consistency (mucoceles are soft)
- The lesion recurrs in the exact same spot repeatedly after rupture
- You have a ranula that is growing (can threaten the airway)
- There is no history of trauma (makes other diagnoses more likely)
Emergency Situations
Seek immediate medical care if:
- A ranula (floor-of-mouth cyst) suddenly enlarges and causes difficulty breathing
- The cyst becomes red, hot, and painful (signs of infection)
The 2-Week Rule
A good general rule for any oral lesion: If it does not heal or significantly improve within 2 weeks, have it evaluated. While most will be benign mucoceles, this rule helps catch the rare dangerous lesions early.
Part 10: Summary – Key Takeaways
Here is everything you need to remember about oral mucoceles:
| Question | Answer |
|---|---|
| What is it? | A benign, fluid-filled cyst from a damaged salivary gland |
| Common symptoms? | Soft, bluish/pink dome-shaped bump; usually painless |
| Is it cancer? | No. Oral mucocele cancer is not a real diagnosis. But other cancers can mimic mucoceles. |
| Will it go away? | Often yes, within 3-6 weeks |
| Should I pop it? | Never. This causes infection and scarring. |
| What treatments work? | Observation, cryotherapy, laser, or surgical excision |
| How to prevent? | Stop lip biting; quit smoking; good oral hygiene |
The Bottom Line
An oral mucocele is almost always a benign nuisance, not a medical emergency. Most will resolve on their own with simple oral mucocele supportive therapy like warm salt water rinses and avoiding further trauma.
However, if you have a persistent, large, or painful oral lesion—or if you are simply worried—see a dentist or doctor. A quick examination can rule out the rare possibility of early stage oral mucocele cancer (more accurately, an early stage salivary gland cancer mimicking a mucocele) and provide peace of mind.
For recurrent or bothersome oral mucoceles, professional oral mucocele treatment—ranging from laser therapy to oral mucocele surgery—offers excellent outcomes with low recurrence rates.
Remember: Your mouth is a window to your overall health. When in doubt, get it checked out.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider for diagnosis and treatment of any oral lesion. Do not attempt to self-treat or self-diagnose oral mucoceles.