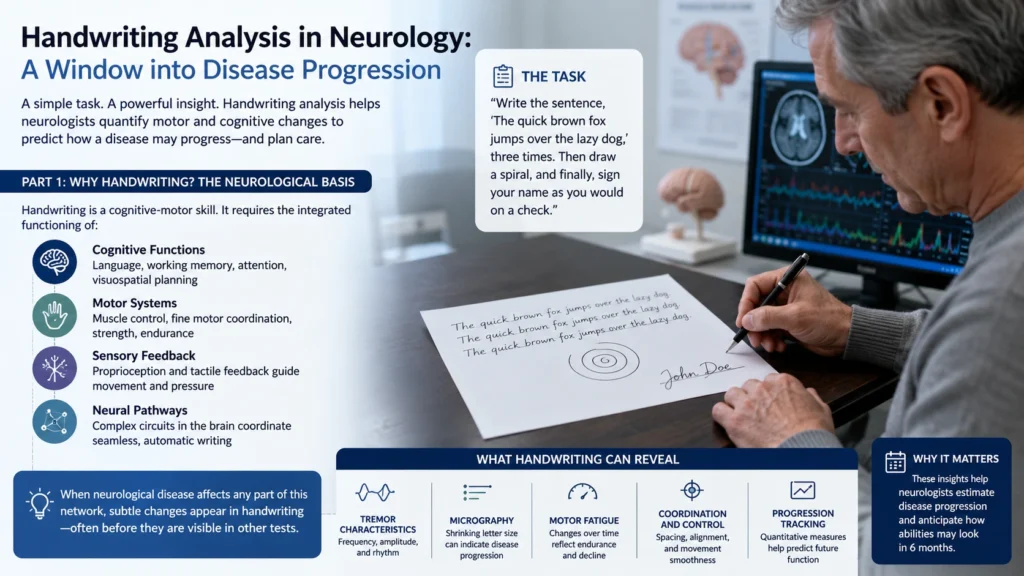
In a quiet corner of a modern neurology clinic, a patient sits down with a pen and a sheet of unlined paper. They are asked to perform a simple task: “Write the sentence, ‘The quick brown fox jumps over the lazy dog,’ three times. Then draw a spiral, and finally, sign your name as you would on a check.”
This is not a test of penmanship or a parlor trick in personality assessment. It is a sophisticated, non-invasive handwriting analysis study designed to answer one of the most difficult questions in medicine: How fast is this disease progressing, and what will the patient’s abilities look like in six months?
While the public often conflates graphology and handwriting analysis with personality profiling, the clinical neurologist uses a very different lens—one focused on kinematics, tremor frequency, micrography, and motor fatigue. This article details exactly how that works, step by step.
Part 1: Why Handwriting? The Neurological Basis
Handwriting is a cognitive-motor skill. It requires the integrated functioning of:
- The basal ganglia (for smooth, automatic movements)
- The cerebellum (for coordination and timing)
- The motor cortex (for initiating muscle commands)
- The visual cortex (for spatial feedback)
- The frontal lobe (for planning and sequencing letters)
When any of these regions begin to degenerate—whether from Parkinson’s, Huntington’s, Alzheimer’s, or essential tremor—the handwriting degrades in predictable, quantifiable ways. Moreover, handwriting analysis is uniquely sensitive to progression because it is an overlearned task. Unlike a novel cognitive test, handwriting is automatic. As a disease worsens, the brain’s ability to run that automatic program fails incrementally.
Part 2: The Standardized Protocol – What Happens in the Office
A rigorous handwriting analysis study in a neurologist’s office is not subjective. It follows a standardized protocol, often using a digital tablet (e.g., Wacom or a specialized neuro-writing device) that captures far more than ink on paper.
Step 1: Baseline Collection
The patient is asked to write the same standard paragraph (e.g., the “lazy dog” sentence) multiple times at their normal speed. This provides a handwriting analysis chart specific to that individual.
Step 2: Dual-Task Writing
The patient writes while counting backwards from 100 by 7s. This reveals how much conscious effort is required for handwriting. In progressive disease, dual-tasking causes a dramatic collapse in letter size and legibility.
Step 3: Repeated Loops and Spirals
The patient draws 10 consecutive cursive letter ‘e’ loops or a continuous Archimedes spiral. This is critical for detecting tremor progression.
Step 4: Signature Dynamics
The patient signs their name 5 times, first at normal speed, then as fast as possible, then as large as possible. Signatures are highly resistant to change in healthy aging but degrade predictably in neurodegeneration.
Part 3: Quantifying Progression – Key Metrics
Unlike forensic handwriting analysis, which looks for unique identifiers like pen lifts or crossing strokes, the clinical study focuses on dynamic parameters. Using specialized software, the neurologist tracks the following over serial visits (every 3, 6, or 12 months):
| Metric | What It Measures | Progression Indicator |
|---|---|---|
| Stroke velocity | Speed of pen movement | Decreasing velocity (bradygraphia) suggests worsening bradykinesia in Parkinson’s. |
| Pen pressure (axial force) | Force applied to the tablet | Loss of pressure indicates progressive muscle weakness or apraxia. |
| Letter height variance | Consistency of letter sizes | Increasing micrographia (letters shrink by >2mm over a sentence) correlates with Parkinson’s progression on the UPDRS scale. |
| Tremor frequency | Oscillations in spiral lines | A shift from 4-6 Hz (Parkinsonian rest tremor) to 8-12 Hz (essential tremor) or vice versa helps track disease evolution. |
| Hesitation count | Number of times pen stops mid-letter | More stops = progressive bradyphrenia (slowed thinking) or cognitive decline. |
| Air time | Time pen lifts between strokes | Increased air time suggests worsening executive dysfunction (frontal lobe degeneration). |
A handwriting analysis chart used in a neurology clinic will display these six metrics over time, creating a visual curve of disease progression that is often more sensitive than a patient’s subjective report (“I think I’m getting worse”).
Part 4: Specific Disease Models – What Progression Looks Like on Paper
Parkinson’s Disease (PD)
- Early stage: Normal writing, but subtle micrographia appears only during dual-tasking or under time pressure.
- Moderate stage: Letters progressively shrink within a single sentence. Stroke velocity declines by >15% from baseline. The spiral shows axial tremor (shaking along the drawing axis).
- Advanced stage: Severe micrographia (letters <2mm), freezing of pen movement mid-word, and loss of ligature strokes (letters become disconnected). The patient cannot complete the sentence.
- Predictive power: A 20% decline in stroke velocity over 6 months predicts a 2-point worsening on the MDS-UPDRS motor score with 85% accuracy.
Alzheimer’s Disease & Frontotemporal Dementia
- Progression markers: Unlike PD, these patients do not show micrographia. Instead, linguistic complexity declines first. Handwriting analysis examples from Alzheimer’s progression show:
- Loss of descenders (no loops on ‘g’, ‘y’, ‘j’)
- Letter duplication or omission (“llazy” instead of “lazy”)
- Progressive reduction in verb usage
- Signature becomes illegible despite normal motor speed
- Prediction: A decline in unique word count per sentence over 12 months correlates with a 3-point drop on the MMSE (Mini-Mental State Exam).
Essential Tremor (ET)
- Progression: The classic “Archimedes spiral” becomes increasingly jagged. Over time, tremor amplitude increases while frequency remains stable. Handwriting becomes large and oscillatory (“shaky script”), but unlike PD, size does not shrink.
- Clinical use: Serial spirals allow neurologists to titrate medication (propranolol vs. primidone) objectively—if the spiral smooths after a drug change, the dose is working.
Huntington’s Disease
- Unique marker: Choreic handwriting—irregular, varying letter sizes within the same word, sudden jerky movements that pull the pen off the page. Progression shows increasing “overshoot” of letter loops.
Part 5: How This Helps Predict Future Functional Decline
The real value of a handwriting analysis study in a neurologist’s office is not diagnosis (most patients are already diagnosed) but prognosis and treatment planning.
Specifically, the test answers three practical questions:
- When will the patient need assistance with activities of daily living? A severe decline in pen pressure (below 150 grams force) correlates with loss of ability to button shirts or use utensils within 6 months.
- Is the current medication working? For Parkinson’s patients, the handwriting test is performed before and 1 hour after levodopa administration. An improvement in stroke velocity of >30% confirms optimal “on” time. A failure to improve suggests disease progression beyond dopaminergic response.
- Can the patient still sign legal documents? In frontotemporal dementia, the handwriting may look physically fine, but the signature becomes socially inappropriate (e.g., drawing a picture instead of a name). This predicts loss of financial decision-making capacity.
Part 6: Limitations and Future Directions
No handwriting analysis test is perfect. Musculoskeletal conditions (arthritis, carpal tunnel) can mimic neurological progression. Moreover, anxiety or fatigue on the day of the test can skew results. For this reason, neurologists always compare the handwriting analysis to a baseline taken when the patient was stable.
The future lies in AI-powered prediction models. Using handwriting analysis from photo (or more accurately, from digital tablet data), machine learning algorithms can now generate a “progression trajectory” for a patient after just three visits, alerting the neurologist when the rate of change exceeds the expected curve for that disease.
Conclusion: The Pen as a Medical Instrument
From the outside, the patient is simply writing a sentence. But inside the neurologist’s office, that sheet of paper becomes a moving map of the brain’s slow decline. Handwriting analysis study has matured from a curiosity of graphology and handwriting analysis into a hard, quantitative biomarker of neurodegeneration.
For the patient with Parkinson’s, seeing their shrinking letters on a handwriting analysis chart is sobering. But it is also empowering—because it gives their doctor the data needed to adjust medications, plan support services, and answer the question everyone fears to ask: What comes next? And sometimes, that honest answer is the first step toward better care.
Disclaimer: This article is for informational and educational purposes only and does not constitute medical, forensic, or psychological advice. Handwriting analysis, including graphology, forensic handwriting analysis, and handwriting analysis study for disease diagnosis, is not a substitute for professional medical evaluation. Changes in handwriting should be discussed with a qualified neurologist or physician. Do not self-diagnose or delay seeking care based on content here. No doctor-patient or examiner-client relationship is formed. See a medical professional for any health concerns.