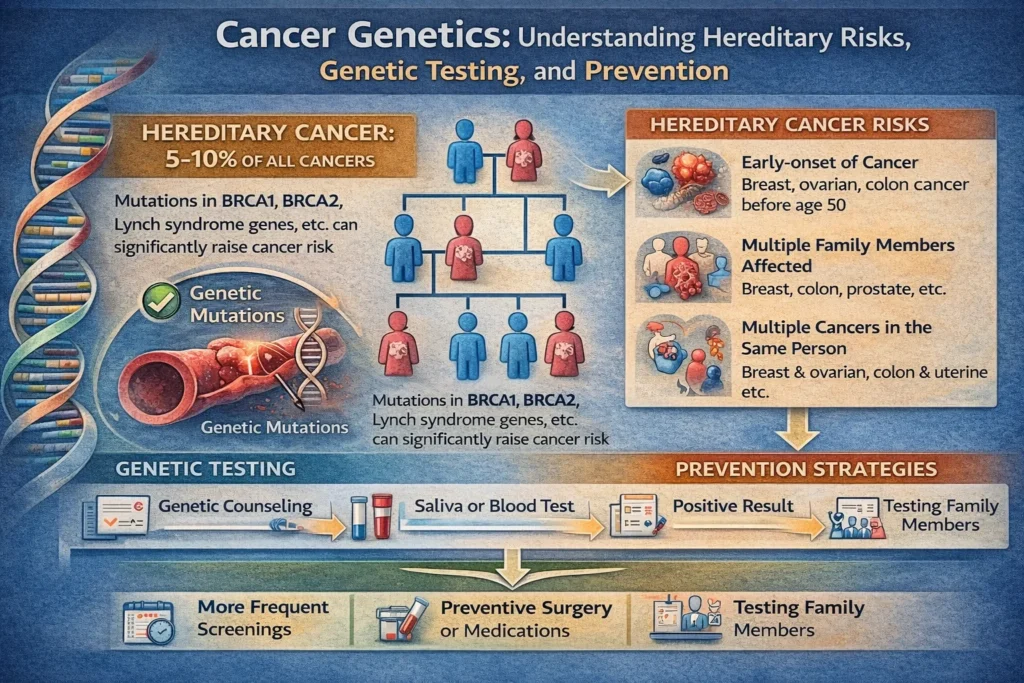
Cancer is a disease of the genes. At its core, every cancer—whether it arises sporadically or runs in families—is caused by changes (mutations) in genes that control how cells grow, divide, and die. However, only about 5-10% of all cancers are inherited. The remaining 90-95% are sporadic, caused by mutations that accumulate over a lifetime due to aging, environmental exposures, or random errors in cell division.
Understanding cancer genetics empowers individuals and families to assess their true risk, pursue appropriate screening, and even take preventive measures. This article explains the fundamentals of hereditary cancer syndromes, the role of genetic counseling and testing, and how to interpret your family history.
Part 1: The Basics – Genes, Mutations, and Cancer
What Are Genes?
Genes are segments of DNA that serve as instruction manuals for making proteins. These proteins control everything from cell growth and division to DNA repair and cell death. Humans have approximately 20,000-25,000 genes.
How Do Mutations Cause Cancer?
A mutation is a permanent change in the DNA sequence of a gene. Mutations can be:
- Inherited (germline): Present in every cell of the body from birth and can be passed to children.
- Acquired (somatic): Occur during a person’s lifetime in a single cell or group of cells and cannot be passed to offspring.
For a normal cell to become cancerous, it typically requires multiple mutations in different types of genes:
| Gene Type | Function | Effect When Mutated |
|---|---|---|
| Oncogenes | Promote cell growth and division | Become overactive (like a stuck accelerator) |
| Tumor Suppressor Genes | Slow down cell division, repair DNA, or trigger cell death | Become inactivated (like failed brakes) |
| DNA Repair Genes | Fix mistakes made during DNA replication | Lead to genomic instability and more mutations |
Classic examples include:
- BRCA1 and BRCA2: Tumor suppressor genes; mutations increase risk of breast, ovarian, pancreatic, and prostate cancers.
- TP53: The “guardian of the genome”; mutations cause Li-Fraumeni syndrome.
- KRAS: An oncogene; mutations drive many lung, colorectal, and pancreatic cancers.
Part 2: Inherited Cancer Syndromes – When Cancer Runs in the Family
Inherited cancer syndromes are caused by germline mutations that significantly increase the risk of developing specific types of cancer, often at younger ages than sporadic cases.
Hallmarks of a Hereditary Cancer Syndrome
- Early age of onset (e.g., breast cancer before age 50)
- Multiple family members on the same side with the same or related cancers
- Bilateral or multiple primary cancers in the same individual (e.g., both breasts, or breast and ovary)
- Rare cancers (e.g., male breast cancer, ovarian cancer, adrenocortical carcinoma)
- Specific ethnic backgrounds (e.g., Ashkenazi Jewish ancestry for BRCA mutations)
Common Hereditary Cancer Syndromes
| Syndrome | Associated Genes | Cancers Most Commonly Associated |
|---|---|---|
| Hereditary Breast and Ovarian Cancer (HBOC) | BRCA1, BRCA2, PALB2, BRIP1, RAD51C, RAD51D | Breast, ovarian, fallopian tube, primary peritoneal, pancreatic, prostate (BRCA2), melanoma |
| Lynch Syndrome (Hereditary Non-Polyposis Colorectal Cancer – HNPCC) | MLH1, MSH2, MSH6, PMS2, EPCAM | Colorectal, endometrial (uterine), ovarian, gastric, small bowel, pancreatic, biliary tract, brain (glioblastoma), sebaceous skin tumors |
| Li-Fraumeni Syndrome (LFS) | TP53 | Soft tissue sarcoma, osteosarcoma, breast cancer, brain tumors, adrenocortical carcinoma, leukemia, lung cancer |
| Familial Adenomatous Polyposis (FAP) | APC | Colorectal cancer (hundreds to thousands of polyps), duodenal cancer, desmoid tumors, thyroid cancer |
| Cowden Syndrome (PTEN Hamartoma Tumor Syndrome) | PTEN | Breast, thyroid (follicular), endometrial, kidney, colorectal cancers; benign growths (hamartomas) |
| Peutz-Jeghers Syndrome (PJS) | STK11 | Gastrointestinal polyps and cancers (colorectal, small bowel, stomach), breast, pancreatic, ovarian (sex cord tumors), testicular (Sertoli cell) |
| Hereditary Diffuse Gastric Cancer (HDGC) | CDH1 | Diffuse (signet ring) gastric cancer, lobular breast cancer |
| Von Hippel-Lindau (VHL) Syndrome | VHL | Renal cell carcinoma (clear cell), hemangioblastomas (brain, spine, retina), pheochromocytoma, pancreatic cysts/neuroendocrine tumors |
| Multiple Endocrine Neoplasia (MEN1 & MEN2) | MEN1, RET | Parathyroid adenomas, pancreatic neuroendocrine tumors, pituitary adenomas (MEN1); medullary thyroid cancer, pheochromocytoma (MEN2) |
Part 3: Genetic Counseling – The First Step Before Testing
Genetic counseling is a critical process that helps individuals understand their personal and family risk of hereditary cancer. It is not the same as genetic testing. Counseling should occur both before and after testing.
What Happens During Genetic Counseling?
- Risk Assessment: A certified genetic counselor or medical geneticist takes a detailed three-generation family history (pedigree) to identify patterns suggestive of a hereditary syndrome.
- Education: The counselor explains the basics of cancer genetics, the specific syndrome being considered, and the implications of possible test results.
- Informed Consent: The counselor discusses the benefits, limitations, and potential psychosocial impacts of testing.
- Testing Coordination: If the patient chooses to proceed, the counselor orders the appropriate test (often a multi-gene panel).
- Result Disclosure and Management: The counselor interprets the result and discusses medical management options (increased screening, risk-reducing surgery, chemoprevention).
Who Should Consider Genetic Counseling?
Professional guidelines (NCCN, ASCO, NSGC) recommend genetic counseling for individuals with:
- A personal history of cancer at an unusually young age
- Multiple primary cancers in the same person
- A family member with a known inherited mutation
- A close relative with a cancer associated with a hereditary syndrome
- Three or more family members on the same side with the same or related cancers
- A rare cancer (e.g., male breast cancer, ovarian cancer, medullary thyroid cancer)
- Ashkenazi Jewish ancestry with a personal or family history of breast, ovarian, or pancreatic cancer
Part 4: Genetic Testing – What It Can and Cannot Tell You
Types of Genetic Tests
| Test Type | Description | When Used |
|---|---|---|
| Single-Gene Testing | Looks for mutations in one specific gene | When the family history points strongly to one syndrome |
| Multi-Gene Panel Testing | Simultaneously analyzes multiple genes associated with various hereditary cancers | Most common approach today; cost-effective and comprehensive |
| Whole Exome Sequencing (WES) | Sequences all protein-coding genes (about 1-2% of the genome) | When panel testing is negative but strong family history persists |
| Whole Genome Sequencing (WGS) | Sequences the entire genome (including non-coding regions) | Research setting; rarely used clinically for cancer risk |
Possible Results
| Result | Meaning | What It Does Not Mean |
|---|---|---|
| Positive (Pathogenic/Likely Pathogenic Variant) | A mutation known to increase cancer risk was found | You will definitely get cancer. It means your risk is elevated, not certain. |
| Negative (No Pathogenic Variant Found) | No known disease-causing mutation was detected in the genes tested | You have no genetic risk from the tested genes. You can still develop sporadic cancer. |
| Variant of Uncertain Significance (VUS) | A DNA change was found, but it is not yet known whether it increases cancer risk | This is not a positive result. Most VUS are eventually reclassified as benign. Do not make medical decisions based on a VUS. |
Important Limitations of Genetic Testing
- Not all hereditary cancers have an identifiable gene mutation. A negative test does not rule out a hereditary component.
- Ethnic-specific mutations (e.g., BRCA founder mutations in Ashkenazi Jews) require specific testing approaches.
- Genetic testing cannot predict the exact age of onset or severity of cancer.
- VUS results are common (in up to 40% of panel tests) and require patience and reanalysis over time.
Part 5: Managing Hereditary Cancer Risk
Once a pathogenic mutation is identified, management focuses on early detection and risk reduction.
Increased Surveillance (Screening)
| Gene/Syndrome | Recommended Screening |
|---|---|
| BRCA1/2 | Breast MRI starting at age 25-30; mammography at 30-35; transvaginal ultrasound and CA-125 for ovarian cancer (limited benefit); pancreatic MRI/MRCP and EUS for those with family history; prostate cancer screening (PSA) starting at 40 for BRCA2 |
| Lynch Syndrome | Colonoscopy every 1-2 years starting at age 20-25; endometrial biopsy or transvaginal ultrasound annually starting at age 30-35; upper endoscopy for gastric cancer; urinalysis for urothelial cancer |
| TP53 (Li-Fraumeni) | Whole-body MRI annually; rapid diagnostic workup of any symptoms; breast MRI starting at age 20; colonoscopy every 5 years; brain MRI annually |
Risk-Reducing Surgeries
For the highest-risk mutations, preventive surgery dramatically reduces cancer incidence.
| Procedure | Gene | Risk Reduction |
|---|---|---|
| Risk-Reducing Mastectomy (Bilateral) | BRCA1/2, TP53, PTEN | Reduces breast cancer risk by 90-95% |
| Risk-Reducing Salpingo-Oophorectomy (RRSO) | BRCA1/2, BRIP1, RAD51C, RAD51D, Lynch (MSH2/6) | Reduces ovarian/fallopian tube cancer risk by 80-96%; also reduces breast cancer risk by 50% if done premenopausally in BRCA carriers |
| Risk-Reducing Hysterectomy | Lynch syndrome (MSH2/6) | Eliminates endometrial cancer risk |
| Prophylactic Colectomy | FAP, Lynch (severe phenotype) | Prevents colorectal cancer |
Chemoprevention
Medications can reduce cancer risk in some high-risk individuals:
- Tamoxifen or Raloxifene: Reduces breast cancer risk by 50% in high-risk women (not specifically for BRCA carriers, but effective)
- Oral Contraceptives: Reduce ovarian cancer risk by 50% in BRCA carriers
- Aspirin: Reduces colorectal cancer risk in Lynch syndrome by 50-60%
Part 6: Sporadic vs. Hereditary – The Majority of Cancers
It is crucial to understand that most cancers are not inherited. The vast majority (90-95%) are sporadic, meaning they occur due to acquired mutations from:
- Aging: The longer you live, the more opportunities for random DNA replication errors.
- Environmental Exposures: Tobacco smoke (lung, bladder, head/neck), UV radiation (skin), asbestos (mesothelioma), radon (lung), aflatoxin (liver).
- Lifestyle Factors: Diet, alcohol consumption, obesity, physical inactivity.
- Infectious Agents: HPV (cervical, oropharyngeal), Hepatitis B/C (liver), H. pylori (stomach), EBV (lymphoma, nasopharyngeal).
How to Distinguish: The “Red Flags” for Hereditary Cancer
| Feature | Sporadic Cancer | Hereditary Cancer |
|---|---|---|
| Age of onset | Typically older (>60) | Often younger (<50) |
| Family history | No or minimal family history | Multiple relatives on same side with related cancers |
| Multiple primaries | Rare | Common (bilateral breast, breast+ovary, colon+endometrial) |
| Associated cancers | None specific | Pattern of syndrome-specific cancers |
| Ethnicity | Any | Certain mutations enriched in specific groups (Ashkenazi, Icelandic, Finnish) |
Part 7: Genetic Testing for Cancer Treatment – Precision Oncology
Beyond risk assessment, cancer genetics now plays a vital role in treating existing cancers. Tumor genomic profiling (somatic testing) identifies mutations within the cancer itself, guiding targeted therapies.
Examples of Targeted Therapy Based on Tumor Genetics
| Gene Mutation | Cancer Type | Targeted Therapy |
|---|---|---|
| BRCA1/2 | Ovarian, breast, pancreatic, prostate | PARP inhibitors (olaparib, niraparib, rucaparib) |
| EGFR | Non-small cell lung cancer | EGFR inhibitors (osimertinib, gefitinib, erlotinib) |
| KRAS G12C | Lung, colorectal | Sotorasib, adagrasib |
| BRAF V600E | Melanoma, colorectal, thyroid | BRAF inhibitors (vemurafenib, dabrafenib) + MEK inhibitors |
| HER2 amplification | Breast, gastric, colorectal | Trastuzumab, pertuzumab, T-DM1, T-DXd |
| NTRK fusion | Multiple solid tumors (rare) | Larotrectinib, entrectinib |
| MSI-high (mismatch repair deficiency) | Colorectal, endometrial, other | Immune checkpoint inhibitors (pembrolizumab, dostarlimab) |
| IDH1/IDH2 | Acute myeloid leukemia, glioma | Ivosidenib, enasidenib |
Germline vs. Somatic Testing: Key Difference
| Feature | Germline (Hereditary) Testing | Somatic (Tumor) Testing |
|---|---|---|
| Sample source | Blood, saliva, or buccal swab | Tumor tissue (biopsy or surgical specimen) |
| What it detects | Mutations present in every cell of the body | Mutations acquired only in the cancer cells |
| Purpose | Assess inherited cancer risk; guide prevention | Guide targeted therapy; prognosis |
| Implications for family | Yes – mutations can be passed to children | No – somatic mutations are not inherited |
| When performed | Before cancer diagnosis (risk assessment) or after | At time of cancer diagnosis (for treatment planning) |
Important: If a somatic test reveals a mutation in a gene that can also be inherited (e.g., BRCA, TP53, MLH1), confirmatory germline testing is recommended to determine if the mutation is hereditary.
Part 8: Psychosocial and Ethical Considerations
Genetic testing for cancer risk carries profound emotional, social, and ethical implications.
Potential Psychological Impact
- Anxiety and distress: A positive result can cause fear and uncertainty about future cancer.
- Survivor guilt: Individuals who test negative may feel guilt toward affected family members.
- Family dynamics: Results affect not just the individual but parents, siblings, and children. Decisions about who to inform and when can be difficult.
Ethical and Legal Protections
In the United States, two major laws protect individuals undergoing genetic testing:
| Law | What It Does |
|---|---|
| Genetic Information Nondiscrimination Act (GINA) of 2008 | Prohibits health insurers from using genetic information to determine eligibility, coverage, or premiums. Also prohibits employers from using genetic information in hiring, firing, or promotion decisions. |
| Affordable Care Act (ACA) | Prevents denial of coverage for pre-existing conditions, including hereditary cancer risk. |
Important limitations of GINA:
- Does not apply to life insurance, disability insurance, or long-term care insurance.
- Does not apply to employers with fewer than 15 employees.
- Does not apply to military or Veterans Health Administration.
Genetic Discrimination Remains a Concern
Despite GINA, some individuals choose to pay out-of-pocket for genetic testing (rather than using insurance) to avoid the possibility of discrimination for life insurance or disability insurance. This is a personal decision that should be discussed with a genetic counselor.
Part 9: Special Populations and Considerations
Ashkenazi Jewish Ancestry
Individuals of Ashkenazi (Eastern European) Jewish descent have a 1 in 40 carrier frequency for three specific BRCA founder mutations (185delAG, 5382insC in BRCA1; 6174delT in BRCA2). This is 10x higher than the general population. Population-based screening for these three mutations is recommended by some expert groups regardless of family history.
African Ancestry
Certain hereditary cancer syndromes, such as hereditary breast and ovarian cancer, occur at similar frequencies across racial groups, but testing disparities exist. African American women are less likely to be referred for genetic counseling or to complete testing, even when criteria are met. Efforts to increase equitable access are ongoing.
Men and Hereditary Cancer
Men are often overlooked in cancer genetics discussions, but male BRCA2 carriers have:
- 8-9% lifetime risk of male breast cancer (compared to 0.1% in general population)
- Elevated risk of prostate cancer (more aggressive forms)
- 5-7% risk of pancreatic cancer
Men with Lynch syndrome have high risks of colorectal cancer and other Lynch-associated cancers. Genetic testing is equally important for men.
Pediatric Hereditary Cancer Syndromes
Most hereditary cancer syndromes manifest in adulthood, but some present in childhood:
| Syndrome | Gene | Childhood Cancers |
|---|---|---|
| Li-Fraumeni | TP53 | Soft tissue sarcomas, osteosarcoma, adrenocortical carcinoma, brain tumors |
| Familial Adenomatous Polyposis (FAP) | APC | Colorectal polyps (teenage years), hepatoblastoma (infancy) |
| Retinoblastoma (RB1) | RB1 | Retinoblastoma (eye cancer in young children) |
| DICER1 Syndrome | DICER1 | Pleuropulmonary blastoma, ovarian Sertoli-Leydig cell tumors, thyroid nodules |
Part 10: The Future of Cancer Genetics
The field of cancer genetics is evolving rapidly. Emerging trends include:
1. Polygenic Risk Scores (PRS)
Most cancers are influenced by many common genetic variants, each with a small effect. Polygenic risk scores combine information from hundreds of thousands of these variants to estimate an individual’s risk of developing specific cancers. PRS is not yet ready for routine clinical use but may eventually refine risk assessment for individuals without strong family histories.
2. Liquid Biopsies
Circulating tumor DNA (ctDNA) can be detected in blood samples, allowing for early cancer detection, monitoring of treatment response, and detection of minimal residual disease (MRD) after surgery. Liquid biopsies are already used in some clinical contexts and are being studied for population-based screening.
3. CRISPR and Gene Editing
While still experimental, CRISPR-Cas9 gene editing has been used in clinical trials to edit immune cells to fight cancer (CAR-T therapy) and to correct inherited mutations in laboratory models. Therapeutic gene editing for hereditary cancer risk is not yet available.
4. Population-Based Screening
Some experts now recommend population-based BRCA screening for all women over age 30, regardless of family history. This approach is already implemented in Israel and is being studied in the United States. It would identify many carriers who would otherwise be missed by family-history-based criteria.
Summary Table: Key Takeaways
| Question | Answer |
|---|---|
| What percentage of cancers are hereditary? | 5-10% |
| What are the main types of cancer-related genes? | Oncogenes, tumor suppressor genes, DNA repair genes |
| What is the difference between germline and somatic mutations? | Germline (inherited, in every cell) vs. Somatic (acquired, only in cancer cells) |
| What are the most common hereditary cancer syndromes? | HBOC (BRCA1/2), Lynch syndrome, Li-Fraumeni, FAP, Cowden, PJS |
| Who should consider genetic testing? | Anyone with early-onset cancer, multiple primaries, strong family history, or rare cancers |
| What does a positive test mean? | Elevated risk, not certainty of cancer |
| What does a Variant of Uncertain Significance (VUS) mean? | It is NOT a positive result; do not make medical decisions based on a VUS |
| Can genetic testing results be used against me? | GINA protects against health insurance and employment discrimination, but not life/disability insurance |
| What are the main risk management options? | Increased screening (MRI, colonoscopy), risk-reducing surgery (mastectomy, oophorectomy), chemoprevention |
Conclusion: Knowledge Is Power
Understanding cancer genetics transforms fear into actionable knowledge. For the 5-10% of individuals with a hereditary cancer syndrome, knowing your genetic status allows for:
- Early detection through intensive, personalized screening
- Risk reduction through preventive surgeries or medications
- Family planning decisions (prenatal testing, preimplantation genetic diagnosis)
- Informed participation in cancer prevention clinical trials
For the vast majority without an inherited syndrome, the same knowledge provides reassurance and empowers lifestyle changes to reduce sporadic cancer risk.
If you have a personal or family history suggestive of hereditary cancer, the first step is genetic counseling—not ordering a direct-to-consumer test from an online company. Certified genetic counselors can help you navigate the complex landscape of cancer genetics, interpret results accurately, and develop a personalized risk management plan.
Your genes are not your destiny. But understanding them is your greatest advantage.
Disclaimer: This article is for informational and educational purposes only and does not constitute medical advice. Genetic testing decisions should be made in consultation with a qualified healthcare provider or certified genetic counselor.
Affiliate Note: Interested in learning more about hereditary cancer risk? [Click here to explore books on cancer genetics on Amazon](https://www.amazon.com/s?k=cancer+genetics+books&tag=your affiliate id-20) or find [DNA collection kits for ancestry and health](https://www.amazon.com/s?k=DNA+test+kit+health&tag=your affiliate id-20) (note: these are not substitutes for clinical genetic testing).