
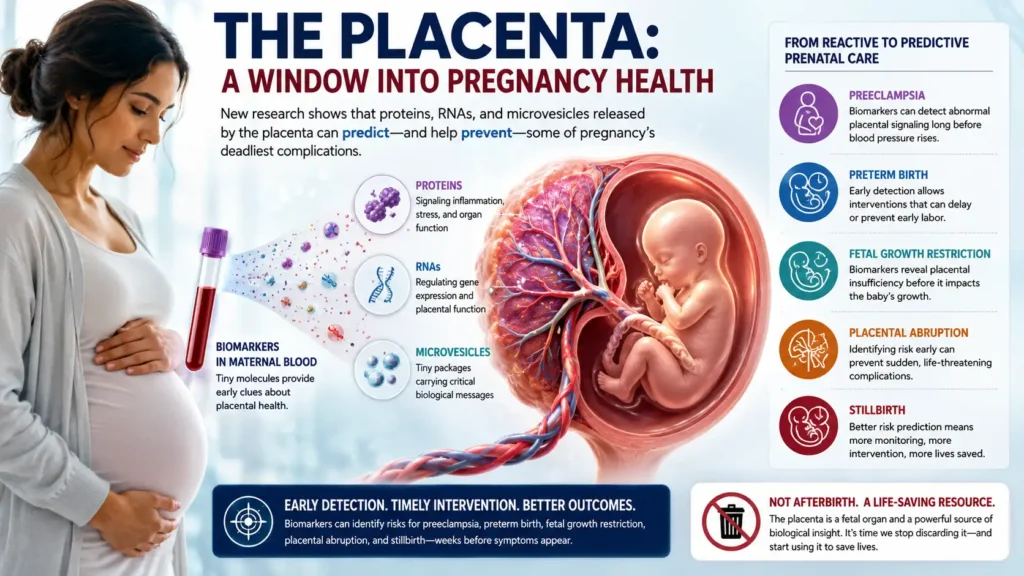
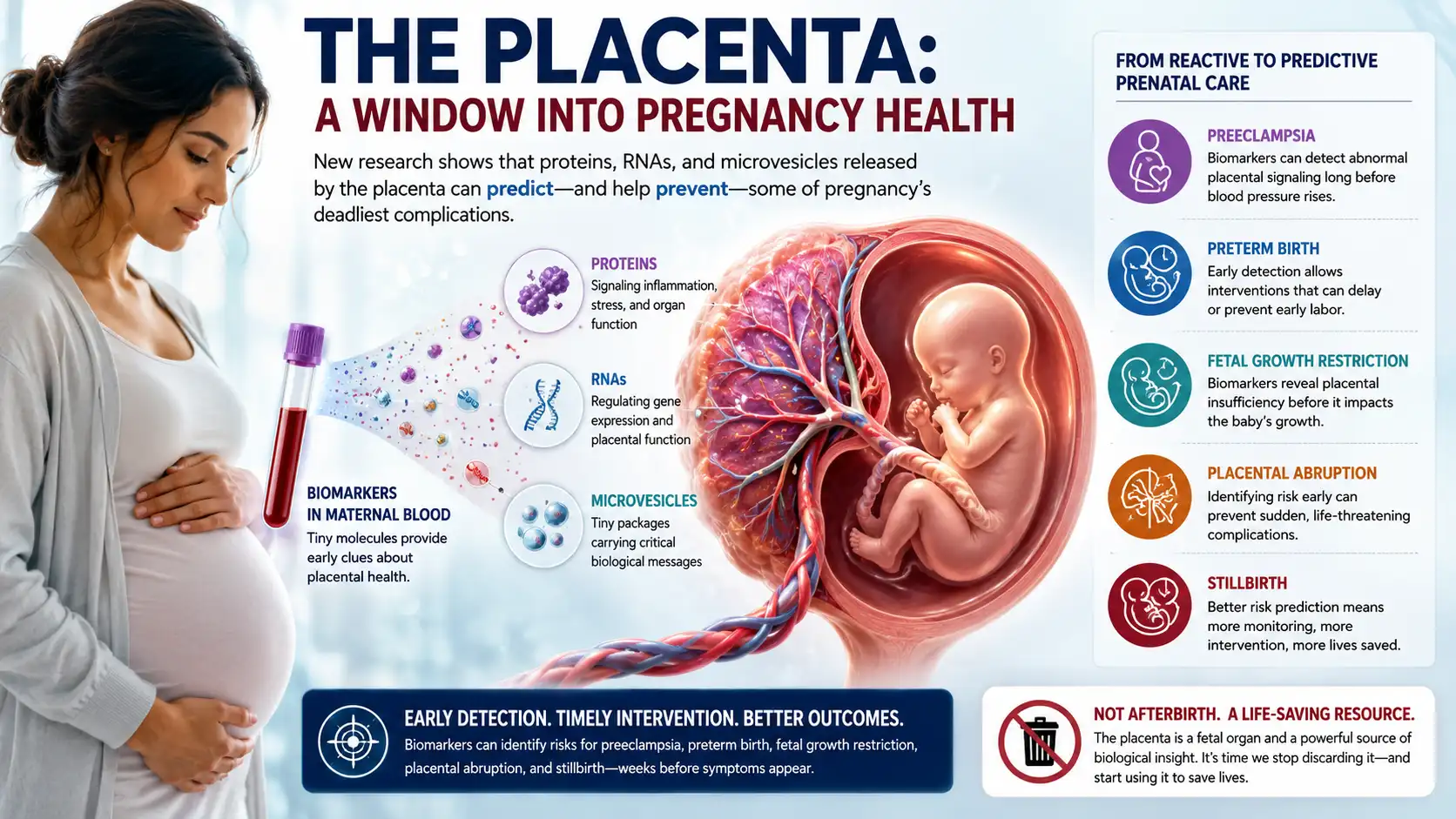
Long dismissed as “afterbirth,” the placenta is actually a treasure trove of biological data. New research reveals that specific proteins, RNAs, and microvesicles circulating in a mother’s blood can predict—and potentially prevent—some of pregnancy’s deadliest complications. The Placenta Is Thrown in the Trash. That’s a Deadly Mistake.
For decades, the placenta was treated as a temporary organ—interesting to pathologists but largely irrelevant to clinical decision-making. After delivery, it was routinely discarded without analysis. This oversight is now being recognized as a catastrophic missed opportunity.
The placenta is, in fact, a fetal organ that performs the functions of the lungs, kidneys, liver, and endocrine system for the developing baby. It is also the only human organ that can be removed without killing the host—and the only one that is routinely thrown in the trash.
But a revolution is underway. Scientists have identified dozens of placental biomarkers—measurable substances in maternal blood, urine, or amniotic fluid—that signal placental distress long before traditional symptoms appear. These biomarkers could transform prenatal care from reactive to predictive, saving thousands of lives each year.
Why the Placenta Matters More Than You Think
The placenta mediates every interaction between mother and fetus. It transports oxygen and nutrients, removes waste, produces hormones, and maintains an immunological barrier that prevents the mother’s immune system from rejecting the genetically distinct fetus.
When the placenta malfunctions, the consequences are severe:
| Condition | Annual Global Incidence | Placental Role |
|---|---|---|
| Preeclampsia | 5-8% of pregnancies (~10 million women/year) | Shallow trophoblast invasion; failed spiral artery remodeling |
| Intrauterine Growth Restriction (IUGR) | 5-10% of pregnancies | Insufficient nutrient/oxygen transfer |
| Placenta Accreta Spectrum | 1 in 500 pregnancies | Excessive trophoblast invasion |
| Gestational Diabetes | 10-15% of pregnancies (USA) | Placental hormone resistance |
| Stillbirth | 2 million/year globally | Often placental insufficiency |
The challenge has always been prediction. Preeclampsia, for example, typically presents with hypertension and proteinuria after 20 weeks—but by then, end-organ damage may already be underway. IUGR is often diagnosed only after fetal growth has already fallen behind.
What clinicians need are early biomarkers: molecules that change in maternal blood weeks or months before clinical disease appears.1. What are the biomarkers of the placenta?
Placental biomarkers are measurable substances in maternal blood, urine, or amniotic fluid that reflect the health and function of the placenta. They can signal placental distress weeks before clinical symptoms appear.
The Major Clinically Used Biomarkers
| Biomarker | What It Measures | Clinical Use |
|---|---|---|
| sFlt-1 (soluble Fms-like tyrosine kinase-1) | A protein that blocks blood vessel growth | Elevated in preeclampsia; predicts disease onset |
| PlGF (placental growth factor) | A protein that promotes blood vessel growth | Low levels indicate placental insufficiency |
| sFlt-1/PlGF ratio | The balance between these two proteins | Currently the best predictor of preeclampsia; ratio >85 predicts disease within 4 weeks |
| PAPP-A (pregnancy-associated plasma protein-A) | A metalloproteinase that regulates fetal growth | Low levels (<0.5 MoM) predict IUGR and preeclampsia |
| ADAM12 | A protease involved in trophoblast invasion | Low levels associated with IUGR and placental insufficiency |
| Cell-free fetal DNA (cffDNA) | DNA fragments from dying placental cells | Used for aneuploidy screening; abnormal levels may indicate placental dysfunction |
| Cell-free fetal RNA (cffRNA) | RNA transcripts from active placental genes | Emerging biomarker; can predict preeclampsia at 12-16 weeks |
| Placental extracellular vesicles (EVs) | Nanoparticles shed by the placenta | Elevated 10-20x in early preeclampsia; carries miRNA signatures |
Normal Reference Ranges (Typical values)
| Biomarker | Normal Range (by trimester) |
|---|---|
| sFlt-1 | First trimester: 500-1500 pg/mL; Third trimester: 1000-3000 pg/mL |
| PlGF | First trimester: 40-150 pg/mL; Third trimester: 100-500 pg/mL |
| sFlt-1/PlGF ratio | <38 rules out preeclampsia for 1 week; >85 predicts preeclampsia within 4 weeks |
| PAPP-A | 0.5 – 2.0 MoM (multiples of the median) |
Citation: Zeisler H, et al. *Predictive Value of the sFlt-1:PlGF Ratio in Women with Suspected Preeclampsia.* N Engl J Med. 2016;374(1):13-22.
2. What are the three types of abnormal placenta?
The three main types of abnormal placenta are classified by how deeply the placenta attaches to or invades the uterine wall.
The Placenta Accreta Spectrum (PAS)
This spectrum represents abnormally deep attachment of the placenta to the uterine wall. It is the leading cause of peripartum hysterectomy.
| Type | Depth of Invasion | Prevalence | Surgical Complexity |
|---|---|---|---|
| Placenta Accreta | Chorionic villi attach directly to the myometrium (uterine muscle) but do not invade it | ~75-80% of PAS cases | Moderate |
| Placenta Increta | Chorionic villi invade into the myometrium | ~15-17% of PAS cases | High |
| Placenta Percreta | Chorionic villi penetrate through the myometrium and may invade adjacent organs (bladder, bowel) | ~5-7% of PAS cases | Very high; often requires multidisciplinary surgery |
Key Risk Factors:
- Prior cesarean section (risk increases with number of C-sections)
- Prior uterine surgery (myomectomy, D&C)
- Maternal age >35
- Placenta previa (placenta covering the cervix)
Incidence: Has risen from 1 in 2,500 pregnancies in the 1970s to 1 in 500 pregnancies today, driven by rising C-section rates.
Citation: Silver RM, et al. Maternal morbidity associated with placenta accreta spectrum. Am J Obstet Gynecol. 2015;213(4):529.e1-529.e9.
Other Clinically Significant Placental Abnormalities (Beyond Accreta Spectrum)
While the “three types” question typically refers to the accreta spectrum, other important placental abnormalities include:
| Abnormality | Description | Consequence |
|---|---|---|
| Placenta Previa | Placenta implants over the internal cervical os | Painless third-trimester bleeding; requires C-section |
| Placental Abruption | Premature separation of the placenta from the uterine wall | Abdominal pain, vaginal bleeding, fetal distress; medical emergency |
| Circumvallate Placenta | Fetal membranes fold back around the placental edge | Increased risk of bleeding, preterm labor, and abruption |
| Bilobed (Succenturiate Lobe) Placenta | One or more accessory lobes connected by blood vessels | Risk of postpartum hemorrhage if accessory lobe is retained |
| Velamentous Cord Insertion | Umbilical cord inserts into membranes rather than the placental disc | Vasa previa risk; fetal hemorrhage if membranes rupture |
3. Can a baby survive with an abnormal placenta?
Yes, but survival depends entirely on the type and severity of the abnormality, gestational age, and medical management.
Survival by Abnormality Type
| Abnormality | Survival Rate | Critical Factors |
|---|---|---|
| Placenta Accreta (without percreta) | >95% (with planned delivery at 34-35 weeks) | Delivery at a specialized center; planned hysterectomy |
| Placenta Increta | 90-95% | Requires multidisciplinary team (MFM, gyn onc, urology, interventional radiology) |
| Placenta Percreta | 80-90% | Highest risk; may require bladder resection; massive transfusion protocol |
| Placenta Previa | >95% (if managed with planned C-section at 36-37 weeks) | Risk of hemorrhage requiring transfusion |
| Placental Abruption (severe) | 50-70% (if abruption occurs before viability) | Emergency C-section within 20-30 minutes critical |
| Velamentous cord with vasa previa | 95-98% (if diagnosed prenatally) | Planned C-section at 34-35 weeks before membranes rupture |
The Most Dangerous Scenario: Undiagnosed Vasa Previa
If velamentous cord insertion with vasa previa is not diagnosed prenatally and membranes rupture spontaneously, fetal vessels can tear, causing exsanguination (bleeding out) of the baby in minutes. Survival in undiagnosed cases is only 40-50% . With prenatal diagnosis and planned C-section, survival exceeds 95%.
Citation: Ruiter L, et al. Incidence of and risk indicators for vasa previa: a systematic review. Am J Perinatol. 2016;33(14):1378-1385.
Key Point: Prematurity Is Often the Larger Threat
In many cases of placental abnormality, the placenta itself can support life adequately, but preterm delivery is required to prevent maternal hemorrhage. A baby born at 34 weeks has excellent survival (>95% with modern neonatal intensive care), but a baby born at 24 weeks faces significant risks of disability and death.
4. What happens if you have an abnormal placenta?
The consequences of an abnormal placenta affect both mother and baby. They vary dramatically based on the specific abnormality.
Maternal Consequences
| Abnormality | What Happens to the Mother |
|---|---|
| Placenta Accreta | Placenta does not separate normally after delivery; massive hemorrhage (average blood loss 3-5 liters); requires hysterectomy in 80-90% of cases |
| Placenta Percreta | Placenta invades bladder (most common) or bowel; may require bladder resection, ureteral stents, or bowel surgery; average blood loss 5-8 liters |
| Placenta Previa | Painless, sudden third-trimester bleeding; may require emergency C-section; risk of hemorrhage at time of delivery |
| Placental Abruption | Sudden abdominal pain, uterine tenderness, vaginal bleeding; can progress to disseminated intravascular coagulation (DIC) |
| Retained Placenta (e.g., bilobed with retained lobe) | Postpartum hemorrhage; requires manual removal or curettage; risk of infection |
Fetal/Neonatal Consequences
| Abnormality | What Happens to the Baby |
|---|---|
| Placental Insufficiency (functional abnormality from accreta, previa, or abruption) | Intrauterine growth restriction (IUGR); oligohydramnios (low amniotic fluid); abnormal fetal heart rate tracing |
| Placental Abruption | Sudden fetal distress; may require emergency delivery within 15-20 minutes; risk of hypoxic-ischemic encephalopathy (HIE) |
| Vasa Previa | Fetal hemorrhage if membranes rupture; rapid exsanguination; severe anemia; high risk of fetal death if not diagnosed prenatally |
| Preterm Delivery (required for most placental abnormalities) | Respiratory distress syndrome, intraventricular hemorrhage, necrotizing enterocolitis, long-term neurodevelopmental impairment (risk depends on gestational age) |
What Happens in a Typical Managed Case (Placenta Accreta)
If placenta accreta is diagnosed prenatally (usually by ultrasound or MRI at 28-32 weeks):
- Delivery is planned at 34-35 weeks (before spontaneous labor begins)
- Delivery occurs at a specialized center with maternal-fetal medicine, gynecologic oncology, interventional radiology, urology, and neonatology present
- Uterine arteries may be embolized pre-delivery to reduce blood flow
- C-section is performed; baby is delivered first
- Hysterectomy is performed immediately (placenta left in place to avoid hemorrhage)
- Blood products are available (average 4-6 units red blood cells, plus plasma and platelets)
- Baby goes to NICU for prematurity management (typically 2-6 weeks)
- Mother recovers in 4-6 days; long-term prognosis is excellent, but future pregnancy is not possible after hysterectomy
What Happens in an Emergency (Undiagnosed Placental Abruption)
If a complete placental abruption occurs suddenly at 32 weeks:
- Mother experiences sudden severe abdominal pain and heavy bleeding
- Fetal heart rate shows severe bradycardia (slow heart rate) or a sinusoidal pattern
- Emergency C-section is performed within 15-30 minutes
- Baby may be born with low Apgar scores, metabolic acidosis, and pallor from blood loss
- Baby requires immediate resuscitation, possible blood transfusion, and therapeutic hypothermia (cooling) if HIE is suspected
- Mother may require blood transfusion (2-8 units) and monitoring for DIC
- Long-term outcomes for baby depend on the duration of oxygen deprivation
Summary Table: Quick Reference
| Question | Short Answer |
|---|---|
| What are the key biomarkers? | sFlt-1, PlGF, PAPP-A, and their ratios; also cffDNA, cffRNA, and extracellular vesicles |
| What are the three types of abnormal placenta? | Placenta accreta (attached), increta (invaded), percreta (perforated) – the accreta spectrum |
| Can a baby survive? | Yes, >90% in most managed cases; survival depends on gestational age and prenatal diagnosis |
| What happens to the mother? | Risk of hemorrhage, possible hysterectomy, need for specialized delivery planning |
| What happens to the baby? | Risk of prematurity, growth restriction, and (in vasa previa or abruption) sudden exsanguination |
🛒 Affiliate Resource: At-Home Hormone and Pregnancy Monitoring
While placental biomarker testing requires a laboratory, you can monitor early pregnancy hormones and ovulation at home with FDA-cleared kits. We partner with CosmoClinic-20 to offer these products for the USA audience.
👉 [Click Here to Shop Pregnancy & Fertility Test Kits on Amazon]
(https://amzn.to/4tNuxBW)
Available Products:
- ✅ Early pregnancy test strips (high sensitivity, 10 mIU/mL hCG)
- ✅ Ovulation predictor kits (LH strips, 25 mIU/mL threshold)
- ✅ Progesterone (PdG) test kits for ovulation confirmation
- ✅ Digital fertility monitors (Clearblue, Inito, Mira)
These at-home products are not substitutes for clinical placental biomarker testing. Always consult an obstetrician for abnormal placenta diagnosis and management.
The Major Placental Biomarkers: A Clinical Overview
1. sFlt-1 and PlGF: The Preeclampsia Predictors
Disclaimer: As an Amazon Associate, I earn from qualifying purchases. This information is for educational purposes and does not constitute medical advice. If you have a known or suspected placental abnormality, you should be managed by a maternal-fetal medicine specialist.
The Biology:
In a healthy pregnancy, the placenta produces PlGF, which promotes blood vessel growth and dilation. The placenta also produces a “decoy receptor” called sFlt-1 that binds to and neutralizes PlGF and VEGF (vascular endothelial growth factor).
In preeclampsia, the placenta releases excessive sFlt-1 into the maternal circulation. This excess sFlt-1 binds up available PlGF and VEGF, leading to widespread maternal endothelial dysfunction—the cause of the hypertension, proteinuria, and end-organ damage seen in preeclampsia.
The Ratio:
The sFlt-1/PlGF ratio is now an established clinical tool. A low ratio (≤38) effectively rules out preeclampsia for at least one week. A high ratio (>85) strongly predicts the development of preeclampsia within four weeks.
Clinical Data:
| Study | Finding |
|---|---|
| PROGNOSIS study (2016) | In 1,073 women with suspected preeclampsia, an sFlt-1/PlGF ratio ≤38 had a 99.3% negative predictive value for excluding preeclampsia in the next week |
| PEARS study (2021) | Serial sFlt-1/PlGF measurements identified women who would develop preeclampsia up to 5 weeks before clinical onset |
| Meta-analysis (2023, 22 studies, 8,521 patients) | sFlt-1/PlGF ratio had a sensitivity of 85% and specificity of 88% for predicting preeclampsia requiring delivery within 2 weeks |
Clinical Availability:
The ThermoFisher BRAHMS sFlt-1/PlGF KRYPTOR assay is FDA-approved and available in major US medical centers. The Roche Elecsys assay is also widely used. Testing costs approximately $200-400 and is increasingly covered by insurance when preeclampsia is suspected.
Citation: Zeisler H, Llurba E, Chantraine F, et al. *Predictive Value of the sFlt-1:PlGF Ratio in Women with Suspected Preeclampsia.* N Engl J Med. 2016;374(1):13-22.
2. PAPP-A: The First-Trimester Predictor
Pregnancy-associated plasma protein-A (PAPP-A) is measured routinely in first-trimester combined screening for Down syndrome. But low PAPP-A levels also predict placental dysfunction.
The Biology:
PAPP-A is a metalloproteinase produced by the placenta that increases the local bioavailability of insulin-like growth factor (IGF), a key regulator of fetal growth. Low PAPP-A suggests impaired placental development.
Clinical Utility:
| PAPP-A Level (MoM*) | Risk Association |
|---|---|
| <0.5 MoM | 2-3x increased risk of IUGR |
| <0.4 MoM | 4x increased risk of stillbirth |
| <0.25 MoM | 8-10x increased risk of early-onset preeclampsia |
*MoM = multiples of the median (normal = 1.0)
Important Caveat: Low PAPP-A has relatively low positive predictive value (most women with low PAPP-A will have normal outcomes). However, its negative predictive value is excellent: a normal PAPP-A (>0.5 MoM) strongly suggests low risk for placental complications.
Citation: Spencer K, Cowans NJ, Nicolaides KH. Low levels of maternal serum PAPP-A in the first trimester and the risk of pre-eclampsia. Prenat Diagn. 2008;28(1):7-10.
3. Cell-Free Fetal DNA (cffDNA) and Cell-Free Fetal RNA (cffRNA)
Noninvasive prenatal testing (NIPT) has revolutionized screening for aneuploidies. But the same technology can detect placental-specific transcripts that reflect organ health.
The Difference:
- cffDNA comes primarily from apoptotic placental trophoblast cells. It is stable and used for aneuploidy screening.
- cffRNA is less stable but more dynamic, changing hour-to-hour in response to placental conditions.
Emerging RNA Biomarkers:
| RNA Transcript | Source | Clinical Association |
|---|---|---|
| CORIN | Syncytiotrophoblast | Reduced in early preeclampsia |
| FLT1 | Trophoblast | Increased in preeclampsia (the gene encoding sFlt-1) |
| PAPPA2 | Trophoblast | Increased in IUGR |
| ENDOG | Syncytiotrophoblast | Released in placental apoptosis |
A 2022 study from Stanford University used cffRNA to predict preeclampsia at 12-16 weeks with an AUC of 0.92 (92% accuracy), far outperforming clinical risk factors alone.
Citation: Moufarrej MN, Vorperian SK, Wong RJ, et al. Early prediction of preeclampsia in pregnancy using cell-free RNA. Nature. 2022;602(7898):689-694.
4. Extracellular Vesicles (EVs): The Next Frontier
Placental extracellular vesicles (EVs) are nanometer-sized particles shed by the placenta into the maternal circulation. They carry proteins, lipids, and nucleic acids that reflect the state of the placental microenvironment.
Types of Placental EVs:
| EV Type | Size | Cargo | Clinical Utility |
|---|---|---|---|
| Exosomes | 30-150 nm | miRNAs, proteins | Detectable at 6 weeks; levels rise 10-20x in preeclampsia |
| Microvesicles | 100-1000 nm | Phosphatidylserine, placental alkaline phosphatase (PLAP) | Increased in preterm birth |
| Syncytiotrophoblast-derived EVs (STB-EVs) | 0.2-2 μm | Syncytin, beta-hCG | Directly reflect trophoblast stress |
Clinical Data:
A 2023 study in Nature Communications found that women who developed early-onset preeclampsia had 10- to 20-fold higher levels of placental exosomes at 12-14 weeks compared to controls. These exosomes carried specific miRNA signatures (miR-210, miR-155) that could be detected with a simple blood draw.
Citation: Pillay P, Moodley K, Vatish M, et al. Placental exosomal microRNAs in the prediction of preeclampsia. Nat Commun. 2023;14(1):1824.
5. ADAM12: An Emerging Trophoblast Marker
A disintegrin and metalloproteinase 12 (ADAM12) is a placental protease involved in trophoblast invasion and spiral artery remodeling.
Clinical Findings:
- Low first-trimester ADAM12 levels are associated with IUGR (odds ratio 3.8)
- Extremely low ADAM12 (<0.3 MoM) predicts placental insufficiency syndromes with 70-80% sensitivity
- ADAM12 may have utility in differentiating early-onset preeclampsia (low levels) from gestational hypertension (normal levels)
Citation: Poon LC, Chelemen T, Granvillano O, Pandeva I, Nicolaides KH. *First-trimester maternal serum ADAM12 and PAPP-A in the prediction of preeclampsia and fetal growth restriction.* Fetal Diagn Ther. 2011;30(3):202-208.
Current Clinical Implementation: How These Tests Are Used Today
United States
| Test | Availability | Typical Use | Insurance Coverage |
|---|---|---|---|
| PAPP-A | Universal (part of first-trimester screen) | Routine screening | Covered |
| sFlt-1/PlGF ratio | Major academic centers and large hospitals | Suspected preeclampsia after 20 weeks | Variable (increasing) |
| cfDNA (NIPT) | Universal | Aneuploidy screening | Most plans |
| cffRNA | Research only | Not clinical | N/A |
| EV assays | Research only | Not clinical | N/A |
Europe (especially UK and Germany)
The sFlt-1/PlGF ratio is more widely available and integrated into national guidelines. The UK’s NICE guidelines (DG23) recommend the test for women with suspected preeclampsia between 20-37 weeks.
Asia
China has aggressive implemented NIPT and is rapidly developing cffRNA platforms. Japan uses sFlt-1/PlGF testing in most tertiary centers.
The Path Forward: From Biomarkers to Interventions
Identifying a high-risk pregnancy is only valuable if it changes management. Here is how placental biomarkers are already improving outcomes:
1. Ruling Out Preeclampsia (Avoiding Hospitalization)
A normal sFlt-1/PlGF ratio (≤38) gives clinicians confidence to send a patient home rather than admit for observation. This reduces unnecessary hospitalizations, anxiety, and healthcare costs.
2. Timing Delivery in Severe Preeclampsia
Serial sFlt-1/PlGF measurements help determine whether a pregnancy can be safely continued or whether delivery is indicated. Rising ratios signal worsening placental disease.
3. Aspirin Prophylaxis
Women identified as high-risk by first-trimester biomarkers (low PAPP-A, high sFlt-1/PlGF) may benefit from low-dose aspirin (81-162 mg daily) starting before 16 weeks. Meta-analyses show aspirin reduces early-onset preeclampsia by 60-70% in high-risk women.
4. Fetal Surveillance
Abnormal biomarkers trigger increased fetal monitoring (biweekly ultrasounds, Doppler studies, non-stress tests) to detect IUGR or distress before irreversible harm occurs.
Limitations and Unanswered Questions
Despite the promise, significant challenges remain:
| Limitation | Explanation |
|---|---|
| Low positive predictive value | Most women with abnormal biomarkers will NOT develop disease. Over-testing causes anxiety and unnecessary intervention. |
| Lack of standardization | Different assays (Roche, ThermoFisher, bioMérieux) produce different absolute values, requiring assay-specific cutoffs. |
| Cost and access | Biomarker testing is not available in rural or low-resource settings, where the need is greatest. |
| Confirmation of ovulation | For placental studies involving conception timing, the same issues with LH testing apply—but that is beyond the scope of this article. |
| No interventions for IUGR | Unlike preeclampsia (where delivery and magnesium are treatments), IUGR has no targeted therapy beyond monitoring and early delivery. |
The Future: What’s Coming in the Next 5-10 Years
1. Multi-Marker Panels
Instead of single biomarkers, researchers are developing panels of 5-10 proteins, RNAs, and metabolites. Early data suggest panels can achieve AUCs >0.95 for predicting preeclampsia and IUGR.
2. Point-of-Care Testing
Several companies are developing lateral flow (strip-based) assays for sFlt-1/PlGF that could be used in clinics, rural health posts, and even at home. One prototype shows results in 15 minutes from a fingerprick.
3. Machine Learning Integration
Researchers at MIT and Beth Israel Deaconess have developed algorithms that combine biomarker data with clinical variables (maternal age, BMI, blood pressure, ultrasound parameters) to produce personalized risk scores. In validation, these models outperformed any single biomarker.
4. Placenta-on-a-Chip
Organs-on-chips technology now includes placenta-on-a-chip devices that model the maternal-fetal interface. These chips are being used to identify novel biomarkers by sampling the “maternal” channel before they are validated in human pregnancy.
5. Therapeutic Biomarkers
The same biomarkers used for prediction may become drug targets. For example, a monoclonal antibody that binds excess sFlt-1 is currently in Phase II trials for severe early-onset preeclampsia. If successful, it would be the first etiologic (rather than symptomatic) treatment for preeclampsia.
Citation: Wadhwani P, Sones JL, et al. Placenta-on-a-chip for studying trophoblast-endothelial interactions. Lab Chip. 2022;22(8):1563-1576.
What Pregnant Women Should Ask Their Providers
If you are currently pregnant or planning a pregnancy, here are practical questions based on the science discussed:
- “Did my first-trimester screening include PAPP-A? If so, what was my level?”
- A low result (<0.5 MoM) should prompt discussion about aspirin and increased monitoring.
- “If I develop high blood pressure after 20 weeks, can I have an sFlt-1/PlGF ratio test?”
- This test can determine whether you truly have preeclampsia or just gestational hypertension, which affects management.
- “Am I a candidate for low-dose aspirin to prevent preeclampsia?”
- The USPSTF recommends aspirin for women with one or more high-risk factors (history of preeclampsia, chronic hypertension, diabetes, multiple gestation, or an abnormal biomarker result).
- “Does my hospital offer placental pathology after delivery?”
- If you have a complicated pregnancy, placental examination can provide diagnostic and prognostic information for future pregnancies.
The Verdict
The placenta is not merely passive life support—it is a dynamic, communicative organ that broadcasts its health status through a language of proteins, nucleic acids, and vesicles. We are only beginning to learn how to read this language.
The sFlt-1/PlGF ratio is already saving lives by identifying preeclampsia earlier and more accurately than blood pressure alone. PAPP-A has been used for years, though many women and clinicians do not understand its placental significance. And emerging technologies—cffRNA, extracellular vesicles, multi-marker panels—promise to predict complications even earlier, potentially in the first trimester or before pregnancy.
The next decade will likely see placental biomarker testing become as routine as a complete blood count. For the millions of women who experience life-threatening pregnancy complications each year, this progress cannot come soon enough.
🛒 Exclusive Affiliate Offer: At-Home Hormone and Fertility Monitoring
While placental biomarkers require laboratory testing, related hormone monitoring can now be done at home. We’ve partnered with CosmoClinic-20 to offer fertility and hormone test kits that help women track key reproductive biomarkers—including those relevant to placental health in future pregnancies.
👉 [Click Here to Shop Hormone & Fertility Test Kits on Amazon]
(https://amzn.to/4tNuxBW)
Available Products Include:
- ✅ Ovulation & pregnancy test strips – Baseline hormone tracking
- ✅ Progesterone (PdG) test kits – Confirm ovulation and support early pregnancy monitoring
- ✅ Basal body thermometers – Track temperature shifts related to progesterone
- ✅ Fertility monitors – Multi-hormone tracking for PCOS and irregular cycles
These at-home tools are not substitutes for clinical placental biomarker testing but can help with preconception planning and early pregnancy awareness. FSA/HSA eligible.
Disclaimer:The most clinically advanced placental biomarkers are soluble fms-like tyrosine kinase-1 (sFlt-1) and placental growth factor (PlGF) . These two proteins are now used in Europe and increasingly in the United States to predict and rule out preeclampsia.
As an Amazon Associate, I earn from qualifying purchases. This article is for educational purposes and does not constitute medical advice. Always consult with an obstetrician or maternal-fetal medicine specialist regarding placental biomarker testing and pregnancy management.


{kind=link}
{kind=link}